Transcatheter aortic valve replacement (TAVR) procedures performed using transcarotid (TC) access and transfemoral (TF) access are associated with comparable in-hospital and one-year outcomes, according to a new analysis published in the American Journal of Cardiology.[1] These similarities, researchers wrote, suggest TC access is a safe, effective alternative when TF TAVR is not recommended.
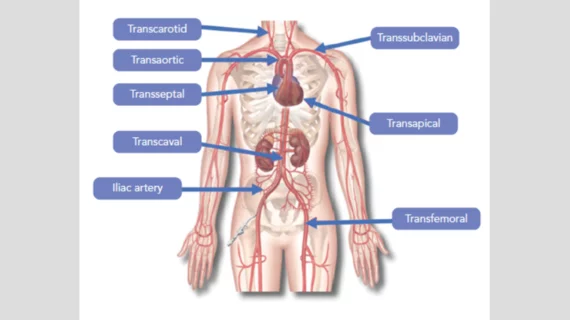
“Despite the availability of lower profile vascular sheaths and valve delivery systems for TAVR, approximately 5% to 15% of patients with TAVR currently require alternative vascular access because of unsuitable iliofemoral anatomy that prevents the use of the conventional TF approach,” wrote first author Nicole E. Hoover, PA-C, of the Hartford HealthCare Heart and Vascular Institute in Hartford, Connecticut, and colleagues. Alternative TAVR access routes that have been described over the last two decades include the transapical, direct aortic, transcaval, subclavian/axillary (TAx) and TC approaches. Although each of these strategies may be suitable for a given patient based on anatomic constraints, there has been a gradual evolution in the use of different alternative access techniques.”
Hoover et al. examined data from than 2,000 TAVR patients treated at a single high-volume medical center. While 1,926 patients with a mean age of 81.3 years old underwent conventional TF TAVR, 138 patients with a mean age of 80.7 years old underwent TAVR using TC access. All patients were treated using current-generation, balloon-expandable or self-expandable TAVR valves. Neuromonitoring was used during every TAVR case that involved TC access.
“Patients were considered for the TC approach if they had unfavorable femoral access either because of inadequate size of the iliofemoral arteries, presence of lower extremity prosthetic grafts, presence of extensive calcification or severe aortoiliac tortuosity, evidence of a hostile groin with infection or rash, or morbid obesity,” the authors wrote.
Overall, no significant differences were seen in the rates of intraprocedural adverse events, in-hospital mortality, one-year mortality or hospital readmission between these two techniques. General anesthesia was used for 26.4% of TF patients and 97.7% of TC patients. Also, TC TAVR procedures took slightly longer than TF TAVR procedures, but they required less contrast.
Hoover and colleagues also noted that multiple prior studies have concluded that the TC approach offers multiple benefits compared to the TAx approach. Perhaps, they wrote, TC access will go on to become the go-to TAVR technique when TF access is not possible.
“The optimal alternative access for patients with TAVR deferred from the traditional TF approach is dependent on the individual patient's anatomic constraints and the previous experience of the surgical team,” the authors wrote. “Although TAx currently remains as the most commonly used alternative access technique, this single-center retrospective analysis … adds to previous reports suggesting that a TC strategy may be considered as the first alternative in patients with contraindications to the femoral route.”

Michael has more than 16 years of experience as a professional writer and editor. He has written at length about cardiology, radiology, artificial intelligence and other key healthcare topics.