Destination Question: Should All STEMI Patients Recover in the ICU?

Two Studies Reach Conflicting Conclusions While Underscoring the Need for Best Practice Guidelines to Fill the Current Vacuum
Over the past 50 years, intensive care units (ICUs) have become an inseparable part of cardiovascular medicine’s dramatic success in reducing deaths from heart attacks. Working hand-in-glove with improvements in reperfusion and adjuvant antithrombotic therapies, ICUs have helped cardiology achieve a nearly 20 percent increase in patient survival over the past 20 years and a significant reduction in complications from STEMI, including cardiogenic shock and life-threatening arrhythmias.
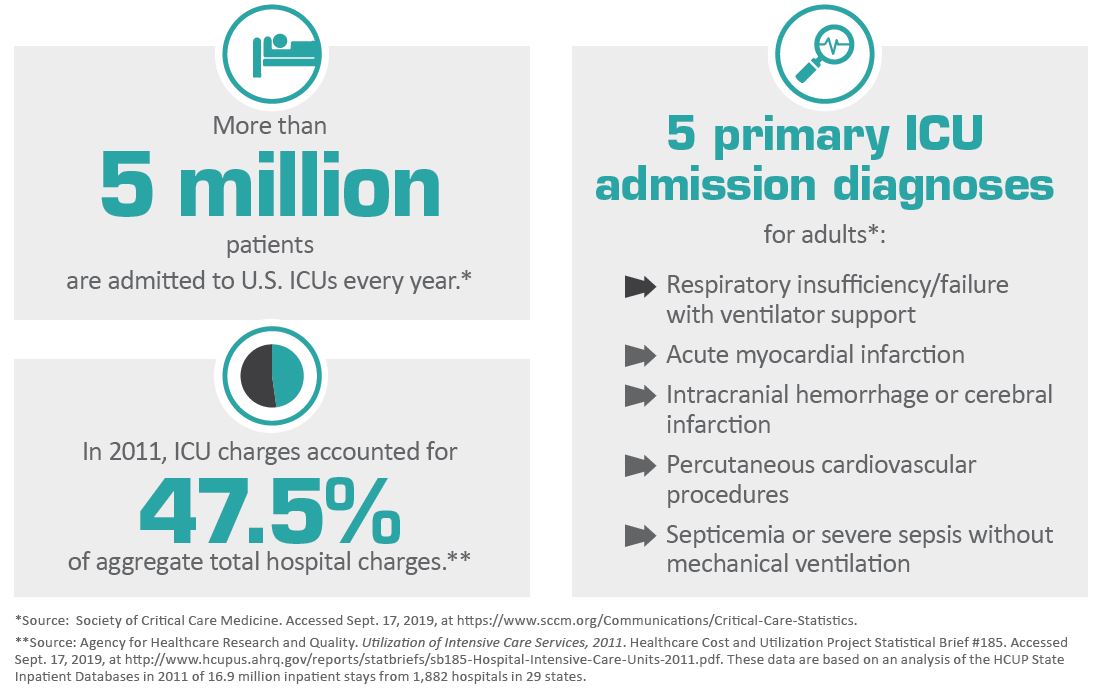
Such numbers are reason for cardiologists and patients to rejoice, but another dataset has begun to rear its troubling head. Despite the fall-off in deaths and complications, the volume of STEMI patients headed to the ICU had not budged. The implications are significant for an increasingly cost-conscious healthcare system where the day rate for an ICU room is around two-and-a-half times the tab for non-ICU admissions and critical care services now account for almost 1 percent of the total U.S. gross domestic product (BMJ 2019;365:I1927). Inevitably, the question has arisen: Is this country’s universal practice of sending the majority of post-PCI patients to the ICU the most effective expenditure of a limited and precious hospital resource?
The argument reached a new pitch earlier this year when a study of hemodynamically stable STEMI patients following reperfusion was published in JACC: Cardiovascular Interventions (2019;12[8]:709-17). Researchers reported that although 82 percent of the nearly 20,000 patients treated at 707 hospitals were referred to the ICU, just 16 percent developed complications requiring an ICU stay, suggesting that intensive care units were being overutilized. Lead author Jay Shavadia, MD, with the Duke Clinical Research Institute in Durham, N.C., told CVB, “There may still exist in a minority of patients a significant risk of developing an ICU-requiring complication, but for the majority of patients who remain uncomplicated a reorganization of STEMI is required given the fact critical care resources are finite and the cost of delivering those resources is substantial.”
For physicians who must wrestle every day with the go-to or don’t-go-to the ICU decision, another comprehensive study this past summer may have compounded the confusion. That paper found that ICU care conferred an absolute survival benefit of 6.1 percent at 30 days for STEMI patients with borderline or discretionary ICU needs vs. admission to other parts of the hospital. What’s more, the authors reported that “efforts to reduce the number of STEMI patients who receive ICU care on average may place [certain populations of at-risk patients] at even higher risk in the future” (BMJ 2019;365:I1927).
“It’s not really a question of underusing or overusing the ICU,” says Thomas Valley, MD, the study’s lead author and assistant professor of internal medicine at the University of Michigan. “The truth is we’re systematically misusing the ICU and need to be better able to target this costly treatment to patients who can actually benefit from it.” As his study puts it, “Whether ICU care for patients with STEMI provides a benefit over lower levels of care, such as general, telemetry, or intermediate care, is poorly understood.”
Victims of their own success
The first coronary care (or intensive care) units for post-MI patients were established in the early 1960s by pioneering cardiologists concerned about the threat of death from malignant arrhythmias. Those units have since become the hub of aggressive critical care for virtually every hospital, safe havens for patients with not just heart disease but co-morbidities that can escalate in the vulnerable period following an MI. Compared to patients in non-ICU units, these patients reap the benefits of enhanced nursing care and, as Valley’s study points out, “more timely access to particular treatments” and to discharge drugs.
In no small way, though, ICUs have become victims of their own success. “Talk to people in any hospital, and they’ll tell you their ICU is full and that they have to ration beds to make room for the really sick patients,” explains Duane Pinto, MD, MPH, a cardiologist at Beth Israel Deaconess Medical Center in Boston. “We’ve filled those beds with post-STEMI patients who don’t really need them, and that creates a very real and practical problem for hospitals today.”
It’s a problem that weighs heavy on the minds of doctors, too. Roxana Mehran, MD, professor of cardiology and population health, science and policy at Mount Sinai Medical Center in New York, frames it this way: “Everyone tries to be cost-conscious, but I think at the end of the day you’re going to err on the side of conservatism because you don’t want to have a complication and loss of life. We’re all aware that in the intensive care unit your patient might have a better chance of survival if something should go wrong.”
Regardless of what side of the ICU fence they’re on, physicians agree that clinical best practice guidelines to replace what are now individual judgments are sorely needed. European guidelines recommend admitting all patients with a STEMI to an ICU (Eur Heart J 2018;39:117-77). Previous American guidelines suggested that STEMI patients at low risk might not need ICU-level care (J Am Coll Cardiol 2004;44:E1-211). Current guidelines are silent on the subject (Circulation 2013;127:e362-425).
There are, of course, certain MI patients who any doctor would agree need acute care recovery. These include patients with rhythm or hemodynamic instability and those who are on ventilators or need mechanical support. But for stable patients who undergo uncomplicated PCI, clinical factors associated with the likelihood of developing ICU-requiring complications are a highly variable set: low systolic blood pressure, high heart rate, elevated initial troponin or serum creatinine, heart failure on first medical contact (FMC), female sex and age, among others.
The study led by Shavadia adds to that list delays in reperfusion (the average time from FMC-to device: 79 minutes) as correlating with a higher rate of complications requiring ICU care (see sidebar). What’s really needed, Shavadia and colleagues say, are risk-based ICU triage strategies “such that patients at high risk for complications are monitored in the ICU and lower risk patients can be safely triaged to lower resource intensity units, such as a telemetry ward.”
“If you’re going to have a STEMI program, you have to be able to take care of the patient in an appropriate way that doesn’t expend resources unnecessarily,” says Pinto, who directs the cardiac catheterization lab at Beth Israel Deaconess Medical Center. “That may mean ramping up expertise on the floor, knowing that your eight-bed ICU might fill up overnight with three heart attacks.” Pinto points out that his hospital maintains a cardiac specialty unit as an alternative to the ICU. There, nurses are trained to recognize and respond quickly to arrhythmias, cardiorespiratory changes and bleeding issues—the complications that physicians worry about most after MI. “Because these nurses are so facile,” Pinto points out, “they enable us to give ICU-level care on the recovery floor.”
In search of a ‘new approach’
In an editorial comment accompanying Shavadia’s study, Suartcha Prueksaritanond, MD, and Amed Abdel-Latif, MD, PhD, both from Gill Heart & Vascular Institute at the University of Kentucky, called for a “new approach” in response to high ICU utilization patterns that would allow “optimal resource utilization to prevail.” That approach, the authors asserted, requires studies challenging outdated practice with “a more comprehensive yet simple-to-follow algorithm for risk stratification of STEMI patients.” Until that occurs, “the ICU admission decision for STEMI patients will continue to be based on individual judgment and traditional protocols rather than robust and evidence-based risk prediction models,” the editorial declared (JACC Cardiovasc Interv 2019;12[8]:718-20).
Well aware of the vacuum that now exists, Valley and his research team are continuing their work aimed at developing guidelines that could be applied broadly across the critical care landscape. “Standardization is a loaded word, but our goal is to reduce unwarranted variation as much as possible,” Valley explains. “If we can identify certain types of patients who benefit from ICU-level care and validate our findings, then we believe those practices will be implemented by most hospitals. Admittedly, ICU care is incredibly costly, but what we want to prevent is the pendulum swinging too far in the direction of keeping patients out of the ICU who truly need its services.”