
Radiation exposure in the cath lab: Tracking the impact on interventional echocardiographers
Interventional echocardiographers performing transesophageal echo (TEE) during structural heart disease (SHD) procedures are exposed to ionizing radiation from their proximity to the cath lab X-ray angiography system. However, there has been limited documentation on the exact exposure levels and what they might mean for overall health.
To answer these questions, researchers with the cardiology department at Teikyo University Hospital in Tokyo, Japan, conducted a study, sharing their findings in the April issue of the Journal of the American College of Cardiology: Asia.[1]
The team found that echocardiographers are exposed to high doses of radiation on the right half of their body, especially the waist and lower body. This is mainly caused by scattered radiation from the bottom edge of the patient bed. The regional dose varied when the C-arm was in different positions. These results suggest that education and appropriate shielding for radiation protection is needed during SHD procedures for echocardiographers, especially young female doctors.
Protective equipment such as mobile, lead-containing acrylic sheets and lead curtains are typically only used by catheter operators in cardiac catheterization suites. The researchers said this means interventional echocardiographers are exposed to a higher radiation dose than the catheter operator in SHD procedures. The study also suggests there is a need for radiation shielding that does not interfere with TEE equipment during SHD procedures.
How much radiation dose is received by interventional echocardiographers?
This study included a retrospective review of dose measures from 79 SHD procedures at the hospital in 2021 that include the use of continuous TEE. This included 44 transcatheter edge-to-edge repair (TEER) procedures of the mitral valve using the MitraClip and 35 transcatheter aortic valve replacements (TAVRs). Personal radiation dosimeters were used to measure the radiation exposure dose at the surface of the interventional echocardiographer’s neck (right side), chest (left pocket location of the radiation protective clothing), and waist (right side). The dosimeters were attached to the outside of the radiation protective clothing. A Monte Carlo simulation was performed to clarify the absorbed dose distribution of radiation on the body surface.
The study also included an observational component using whole-body male phantoms set up in the same position as the echocardiographer in a hybrid cardiac surgery suite. This was used to measure the dose for comparison with the doses recorded during actual procedures.
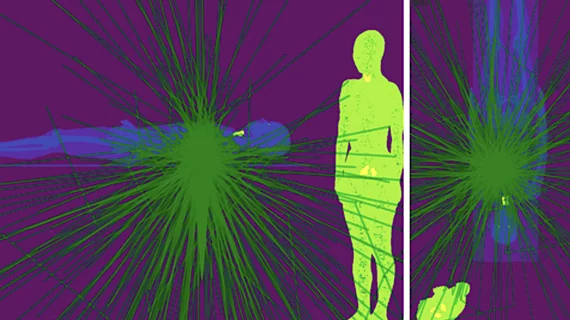
The phantom simulation demonstrated high-dose exposure areas (more than 20 μGy/h) in the right half of the body, especially the waist and lower body. High-dose exposure occurred when obtaining posterior-anterior and cusp-overlap views. The real-life exposure measurements were consistent with the simulation estimates.
Researchers said interventional echocardiographers were more exposed to radiation at their waist in TEER than in TAVR procedures, with a median dose of 0.334 microSieverts/milligray (μSv/mGy) vs. 0.053 μSv/mGy. In TAVR with self-expanding valves compared to balloon-expandable valves, the median dose was 0.067 μSv/mGy vs. 0.039 μSv/mGy, when the posterior-anterior or the right anterior oblique angle fluoroscopic imaging positions were used.
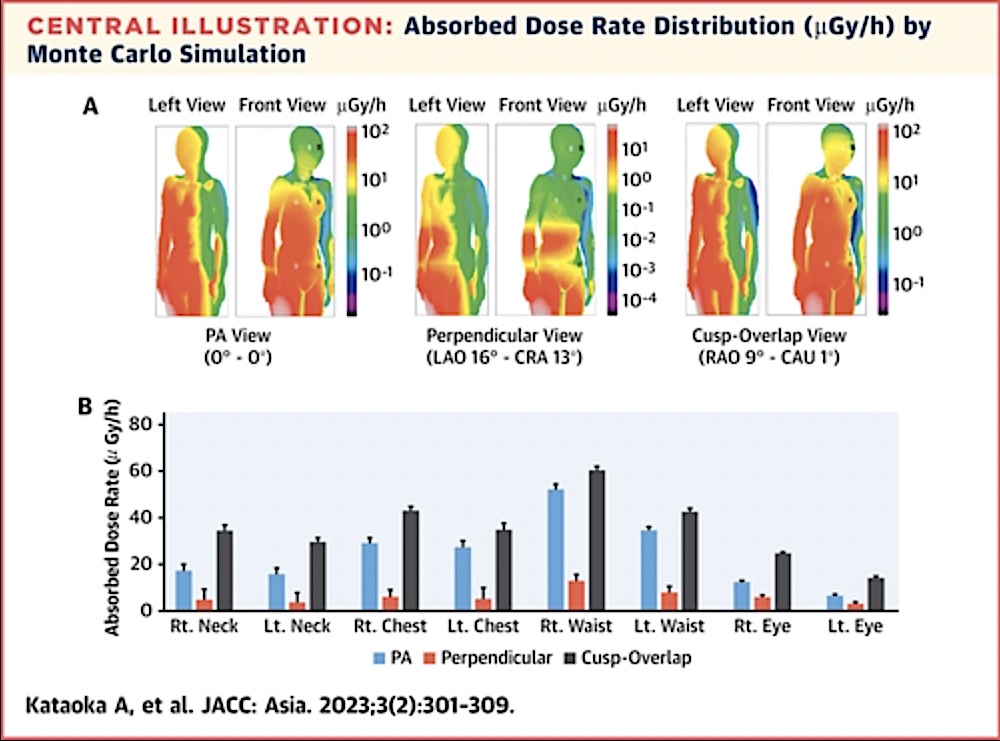
Absorbed X-ray radiation dose rate distribution in microgray per hour (μGy/h) assessed by Monte Carlo simulation for an interventional echocardiographer performing TEE imaging during cath lab structural heart procedures. Read more details.
Overall, greater radiation exposure was found at the waist than at the chest, with a median dose of 11.5 μSv vs. 2 μSv. Differences in the radiation exposure by examine cumulative air kerma (CAK) in the neck, chest and waist were observed between the overall and TEER groups. The overall and TEER groups had higher radiation exposure per CAK at the neck and waist than at the chest. The TAVR group had a higher CAK of 253 mGy vs. 26.2 mGy. TAVR radiation exposure at the chest was 2 μSv vs. 1 μSv for the TEER group. The TEER group had higher radiation exposure per CAK at the neck compared to the TAVR group at 0.222 μSv/mGy vs. 0.027 μSv/mGy, and at the waist was 0.334 μSv/mGy vs. 0.053 μSv/mGy.
Radiation exposure to the eyes and skin in intervention echocardiographers
Radiation-related skin injury is a hazard in various interventional radiology and TAVR procedures, but based on the simulation results in this study, interventional echocardiographers may not reach the radiation dose limit for the skin (500 mSv/y). This suggests that the risk of radiation-related dermatitis or cancer is low.
However, the study found radiation exposure to the eye lenses can increase the risk for developing cataracts, particularly the right eye lens. The use of protective eyewear to reduce lens exposure is therefore recommended, the authors wrote. However, they warned, the interventional echocardiographer is usually at an oblique right anterior position during TEE monitoring, and the radiation could enter the eye through the gap in the eyewear. For this reason, they wrote, appropriate protective eyewear with side protection that securely fits on the face should be used.
TEE is usually performed by echocardiographers, but there are a sizable number of anesthesiologists who also perform TEE during these cardiac procedures.

Dave Fornell has covered healthcare for more than 17 years, with a focus in cardiology and radiology. Fornell is a 5-time winner of a Jesse H. Neal Award, the most prestigious editorial honors in the field of specialized journalism. The wins included best technical content, best use of social media and best COVID-19 coverage. Fornell was also a three-time Neal finalist for best range of work by a single author. He produces more than 100 editorial videos each year, most of them interviews with key opinion leaders in medicine. He also writes technical articles, covers key trends, conducts video hospital site visits, and is very involved with social media. E-mail: dfornell@innovatehealthcare.com