
As Surgery Gives Way to Transcatheter Procedures, Is the Cardiology Cash Cow in Jeopardy?

In her nearly 20 years working closely with patients at the Henry Ford Hospital Heart and Vascular Institute in Detroit, Janet Wyman, DNP, ACNS-BC, has been witness to the seismic change occurring in operating theaters as open-heart surgery yields to transcatheter-based procedures for structural heart disease (SHD).
“Early in my career, I took care of patients in the ICU who had chest tubes and needed intubation and intense pain management, and we weren’t even waking them until the next day,” says Wyman, administrative director of SHD clinical services for Henry Ford Health System, of her aortic valve replacement patients. “Now, with transcatheter replacement, the vast majority go home the next day and 60 minutes after their procedure they’re sitting up in bed smiling and thinking about lunch or dinner. The difference in terms of patient recovery has been dramatic.”
Not just patient recovery, but nearly every facet of cardiovascular care delivery. To be sure, the explosive fields of transcatheter aortic valve replacement (TAVR) and other minimally invasive structural interventions are prompting surgeons to seriously rethink traditional career skills and pathways, societies to investigate changes in how their professionals are trained and accredited, and hospitals to contemplate how sustainable once-sacrosanct business models will be in the face of dwindling surgical valve procedures.
“We’re seeing a sea change driven by the desire for patient-centered care, better outcomes and shorter hospital stays, and by dramatic advances in catheter-based therapies,” says Clifford Kavinsky, MD, PhD, chief of structural and interventional cardiology and director of the Center for Adult Structural Heart Disease at Rush University Medical Center in Chicago. “Hospitals have to recognize this shift is occurring and that standard cardiac surgery, which has always been their cash cow, is going to continue to diminish and lose its preeminent role for them.”
The trend line is captured in the forecasts of industry analysts. According to Frost & Sullivan, the global market for TAVR will double from $3.5 billion in 2018 to between $6 and $7 billion by 2024. “TAVR’s progression to low-risk patients is likely to be a key driver,” reports Sowmya Rajagopalan, global program director for transformational health at Frost & Sullivan. “The growth also is part of the trend we see in the medical device industry to expand market opportunities by application rather than just innovation.” And BCC Research finds that transcatheter mitral valve repair (TMVR) is expected to grow even faster than TAVR, accounting for 22 percent of the global transcatheter valve replacement market by 2023 compared to 12 percent in 2017.
THE MINIMALLY INVASIVE WAVE
Where does this juggernaut leave open-heart surgery? Is it becoming an endangered species? Put the latter question to the field’s experts, and the answer is typically a qualified no.
“I think it’s an evolution, not a revolution,” offers Zoltan Turi, MD, professor of medicine and cardiology at Hackensack Meridian School of Medicine at Seton Hall University in New Jersey.
“It’s just one more step in a minimally invasive process that’s been going on for 40 years with the introduction of coronary angioplasty. There’s no doubt it has affected surgical volumes, but there’s still plenty left for surgeons to do.”
Echoing that thought is Michael Mack, MD, medical director of cardiovascular surgery at Baylor Scott & White Health in Texas, who has notched some 7,000 cardiac procedures over the course of his career, including roughly 800 TAVRs. “What we’re seeing is similar to what happened in vascular surgery over the past 10 to 15 years,” he says, “where the whole field has shifted from mainly open procedures for abdominal aortic aneurysms and peripheral vascular disease to a largely endovascular specialty. This also will happen in cardiac surgery because TAVR is just the first big procedure within structural heart disease that’s shifting. Mitral valve and tricuspid also will gravitate to a transcatheter approach.”
To be sure, mitral valve repair underscores the inexorable movement to percutaneous procedures. Six years after approving MitraClip (Abbott) for degenerative mitral valve regurgitation, the FDA recently expanded the indication to include heart failure patients with moderate-to-severe secondary regurgitation, which is expected to broaden the eligible population to as many as 500,000. Still in its infancy, catheter-based mitral valve repair has already spread to more than 250 hospitals around the country, most of them part of or affiliated with large medical centers.
Minimally invasive tricuspid and pulmonary valve replacement along with patent foramen ovale (PFO) closure to prevent recurrent strokes also are gaining significant clinical ground. Transcatheter techniques to either repair or replace the tricuspid valve, for example, were described in a recent study as “a burgeoning frontier in structural cardiac interventions” (Surg Technol Int 2019;34:321-9). And the TRILUMINATE study of Abbott’s first-of-its-kind device for treating historically difficult tricuspid regurgitation (TR), presented in May 2019 at EuroPCR in Paris, reported that at 30 days 87 percent of patients saw a reduction in TR severity of at least one grade.
So far, no procedure has cut a wider swath across the transcatheter landscape than TAVR. And the prospects for growth are rosier than ever as TAVR migrates to a lower-risk population replete with people determined to avoid open-heart surgery. Two low-risk trials unveiled at ACC.19—PARTNER 3 and SAPIEN 3—informed the FDA’s decision in August to expand the indication for both Medtronic’s Evolut series and Edwards Lifesciences’ Sapien 3 and Sapien Ultra transcatheter heart valves to patients who have severe aortic stenosis and are at low risk for surgery (see related stories: FDA Expands Indication for TAVR to Low-risk Patients and Who Shouldn’t Get TAVR? Lower-risk TAVR Raises New Challenges Around Assessing Patient Eligibility).
As the FDA noted, “At an average of 15-17 months follow-up, when outcomes (such as all-cause mortality or stroke) for transcatheter and surgical patients were compared, the transcatheter heart valve achieved comparable results to surgery, demonstrating a reasonable assurance of safety and effectiveness of the transcatheter heart valves in low surgical risk patients.” Commenting on the trials, one surgeon at the ACC conference remarked, “This is not a paradigm shift, this is a complete flip.”
ARE SPECIALISTS PREPARED FOR CHANGE?
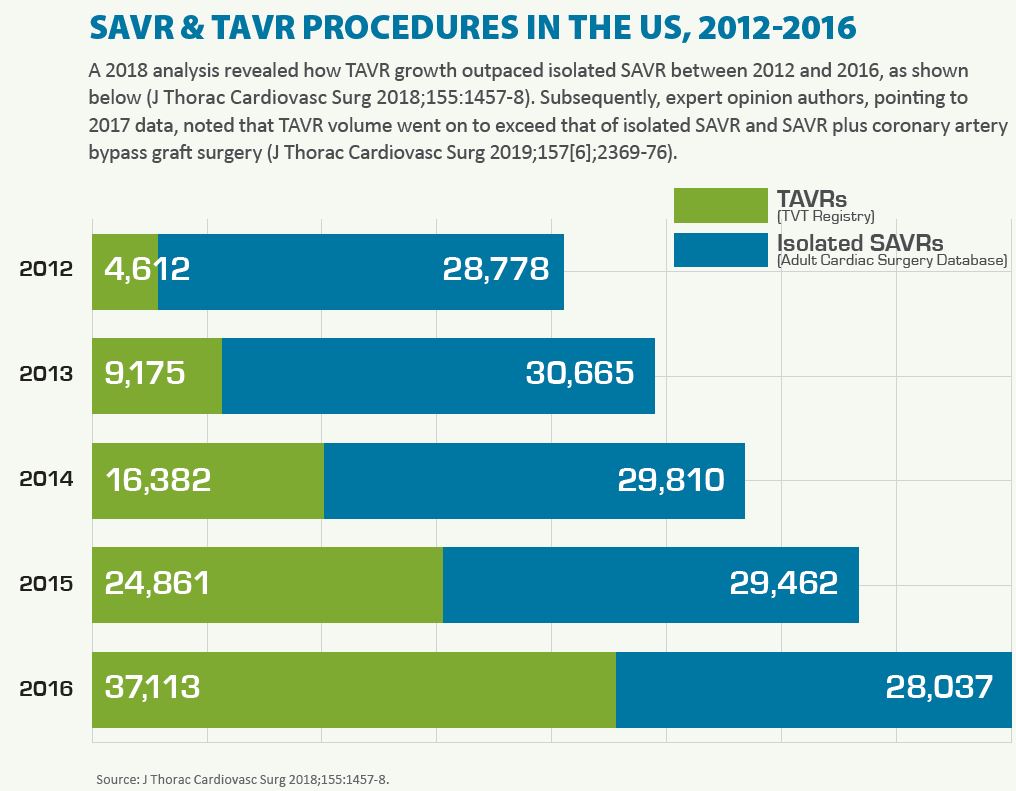
As SAVR volume declines and TAVR increasingly becomes the default for structural valve repair, how can physicians and hospitals prepare for what many in the field envision as a greatly altered state of cardiovascular surgery and patient care?
In June 2019, Mack and others sounded a clarion call for change. “It is increasingly clear that the future of treating SHD will predominantly involve endovascular and minimally invasive techniques,” they wrote in the Journal of Thoracic and Cardiovascular Surgery. “Whether it be cardiologists, surgeons, or both driving the train remains to be seen…. The ‘aha moment’ for our specialty is here; it is the critical time for us to decide what our specialty will look like in the future” (2019;157[6];2369-76).
Certainly, the need for cardiac surgeons will not disappear. A significant number of aortic valve replacements also involve coronary artery bypass grafting (CABG), aortic root replacement and other valve procedures, and these patients usually are better candidates for open-heart procedures. Surgery also may be the only option for patients with anatomic features that preclude TAVR or those for whom transfemoral access isn’t feasible. Mack says the volume of CABG procedures is actually increasing slightly, “and there is a shortage of cardiac surgeons these days.” Even so, the consensus among veterans in the field is that the stable of structural heart specialists needs to grow exponentially in the coming years to meet patient demand.
Kavinsky, who chairs the Structural Heart Disease Council for the Society for Cardiovascular Angiography and Interventions (SCAI), says cardiac surgeons can help fill that need—but only if there is a dramatic change in how they are trained. “They need to acquire the catheter and wire skills of a structural proceduralist if they’re going to participate,” he says. “Those who embrace it and move forward will succeed; those who fight it and try to hold on to the past will be left behind.”
But the pathway to mastery of endovascular skills is anything but inviting for surgeons and residents, given the absence of a standardized, ACGME-accredited training program. Rather, training is fragmented among a small number of non-accredited postgraduate fellowships, mostly at medical centers; on-site device company-sponsored clinical specialist and physician proctorships; and society-sponsored national conferences with interactive live cases and workshops.
“Fellowship training in interventional cardiology is completely focused on coronary intervention,” Kavinsky notes, adding that the technical and cognitive skill sets between the two disciplines vary considerably and can be difficult for surgeons to transition to since percutaneous access usually is not part of their training.
Kavinsky, for one, has been pushing for a formalized, ACGME-accredited fellowship program in SHD interventions that the major societies would support and ACGME would approve with a certification examination by the American Board of Internal Medicine. In their Journal of Thoracic and Cardiovascular Surgery expert opinion, Mack and colleagues put it this way: “Lack of a formalized SHD curriculum results in significant variability in training and exposure making it difficult for surgeons to obtain the full set of required skills to meaningfully participate and contribute during SHD procedures.”
As others peer into the future they don’t see a SAVR vs. TAVR face-off, but rather a hybrid topography where trained specialists move fluidly between the two and turn themselves into valve specialists. “What I foresee for cardiac surgery is that there will be a good interplay between surgery, interventional cardiology and the field of structural heart,” predicts Vinod Thourani, MD, chair of the Department of Cardiac Surgery at MedStar Heart and Vascular Institute in Washington, D.C. “Surgeons will be able to dance seamlessly between those two specialties, whereas today there are only a few of us who routinely do that.”
Thourani, who has performed roughly 2,000 TAVRs and the same number of SAVRs over the past 15 years, practices what he preaches. His handpicked surgical fellows over the past eight years are steeped in both surgery and transcatheter techniques. “My goal for these super-fellows is to develop true equipoise on how they manage valvular disease,” he explains, “so that they can sit down with a patient and say to them, ‘I’m going to do whatever procedure is best for you because I can do both.’”
IMPACT ON HOSPITAL BUDGETS
The TAVR groundswell also is destined to leave an indelible mark on hospitals. An expert consensus paper published in 2019 on the websites of five professional societies prefigures that change, recommending a two-tiered system of valvular heart disease treatment centers—Level 1 (comprehensive valve centers) and Level 2 (primary valve centers)—to account for differences in valve center expertise, experience and resources including imaging (J Am Coll Cardiol 2019;73[20]:2609-35).
According to Kavinsky, this society-backed proposal reflects “a shift away from community hospitals doing cardiac surgery toward large regional medical centers that have the resources to do the full complement of surgery and catheter-based procedures.”
 Even more disruptive for hospitals, though, could be the impact less invasive structural heart procedures have on their business models. These budgets have traditionally been built on a steady and dependable volume of open-heart surgery, whose reimbursement margins far outweigh those of transcatheter procedures. The unavoidable question for administrators thus becomes, will the possible loss of revenue as hospitals shift to TAVR and other structural heart interventions throw them into an economic tailspin?
Even more disruptive for hospitals, though, could be the impact less invasive structural heart procedures have on their business models. These budgets have traditionally been built on a steady and dependable volume of open-heart surgery, whose reimbursement margins far outweigh those of transcatheter procedures. The unavoidable question for administrators thus becomes, will the possible loss of revenue as hospitals shift to TAVR and other structural heart interventions throw them into an economic tailspin?
“The net contribution margin of TAVR is significantly less than it is with surgical aortic valve replacement,” acknowledges Mack. “What you have to measure, though, is the halo effect from being a TAVR center. The profitable procedures you may lose through surgery could be offset by increased imaging studies, diagnostic catheterizations and multiple other procedures and studies that come with TAVR.”
Wyman, of the Henry Ford Hospital Heart and Vascular Institute, which performs more than 300 transcatheter valve replacements annually, also points to the “halo” emanating from TAVR. “We do a CT analysis for all our TAVR patients, but don’t for surgical AVR,” she says, conceding that how hospitals will fare in the brave new world of TAVR remains an intriguing question.
Allowing that margins will be smaller, increased volumes and efficiencies from TAVR could well be offsetting factors, according to Turi. “[TAVR] may not be a cash cow,” he says, “but there are plenty of other places where cardiology is productive both clinically and financially.”
Device durability and cost are the more pressing concerns on Turi’s mind right now. “It’s conceivable that younger patients in their lifetime could have several of these procedures,” he explains, “and it behooves us to raise the uncertainty over durability with them when we discuss treatment options.” Impassioned about cost, Turi says, “TAVR valves are inexcusably expensive,” but he is hopeful that prices will fall “as more companies and devices enter the market.”
In the end, though, patient preference more than anything else could drive the industry’s shift from the surgical to the transcatheter lane. “Patients don’t want big cardiac surgeries anymore,” Kavinsky says. “They want shorter recoveries and shorter hospital stays, and those will dramatically change how we treat many forms of heart disease that have historically relied on invasive, open-heart procedures.”