
A Path for Concurrent Cardiac & Palliative Care

Despite our best efforts to treat the underlying heart disease, people living with advanced cardiovascular disease experience considerable suffering. Heart failure comes with a heavy symptom burden, a complex and unpredictable disease trajectory as well as distress for patients and their families. Such patients are prime candidates for palliative care, a form of interdisciplinary medical care focused on improving quality of life for people living with serious illness and delivered at the same time as management of the underlying disease. Palliative care teams provide an added layer of support for pain and symptom control, psychological and spiritual care, coordination of care and transitions, and skilled communication to elicit patients’ goals of care and support shared decision making.
Both the American College of Cardiology and the American Heart Association recommend that palliative care be integrated into the care of all patients with cardiovascular disease to help relieve symptoms, improve patient satisfaction,
reduce avoidable utilization and costs, and extend survival (Circulation 2016;134[11]:e198-25; J Am Coll Cardiol 2013;128:e240-327). However, studies show that cardiologists seldom refer their patients to palliative care or refer them only in the last days of life (JAMA Netw Open 2019;2[5]:e192375). By taking a few practical steps, cardiologists can partner with colleagues to ensure ongoing identification and management of remediable sources of suffering and distress.
Identify patients with a heavy burden of disease & distress
Patients living with cardiovascular disease should be considered for a palliative care consultation if they meet any of the following criteria: multiple hospital admissions, uncontrolled symptoms, family caregiver burden, a complex home or social situation that makes discharge unsafe or diminished functional and/or cognitive status. This group is at highest risk for repeated emergency department (ED) visits and hospitalizations precipitated by the symptom distress, anxiety and depression typical of progressive heart disease. People with at least one serious illness and functional impairment who also have had one or more hospitalizations or skilled nursing facility stays in the past year have a 47 percent risk of hospitalization and a 28 percent risk of death in the subsequent year (Health Serv Res 2017;52:113 31). Any patient meeting these criteria should be considered for an added layer of support to prevent a cascade of crisis hospitalizations.
Cardiology practices can standardize routine assessment into their workflows by using short validated tools. In the waiting room, pain and symptoms can be screened using the Edmonton Symptom Assessment System; depression and anxiety with the PHQ-4 (Patient Health Questionnaire-4); and family caregiver burden with the Zarit Burden Interview. Patients and their caregivers can be asked to complete these assessments on a tablet, and results can flow directly into the electronic health record (EHR). Cloud-based patient reporting of symptoms via smartphone also can be done from home, enabling early identification of decompensation and the opportunity to avert the next crisis. Triggers can be set in the EHR to alert staff and providers to concerning patient reports, prompting discussion and resolution.
Deliver concurrent palliative & cardiac care
Palliative care can and should be delivered concurrently with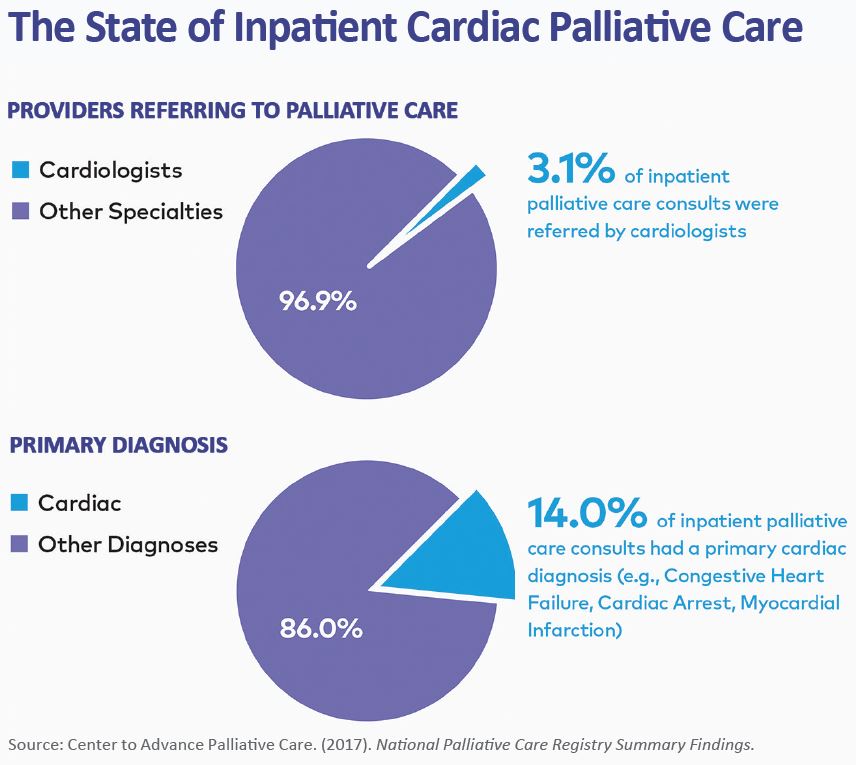 specialist-level cardiac care. With some additional training in safe and effective pain and symptom management and in communications, cardiologists can and should address many of their patients’ sources of distress (pain, dyspnea, fatigue, anxiety, depression) in their own practices. Careful management of heart failure therapies is a critical component of symptom management, but additional strategies for advanced symptom management and communication skills have not yet been integrated into cardiology education. Multiple online courses are available, including through my own organization, the Center to Advance Palliative Care (CAPC). Many cardiologists have free access to CAPC’s online courses through their member organizations.
specialist-level cardiac care. With some additional training in safe and effective pain and symptom management and in communications, cardiologists can and should address many of their patients’ sources of distress (pain, dyspnea, fatigue, anxiety, depression) in their own practices. Careful management of heart failure therapies is a critical component of symptom management, but additional strategies for advanced symptom management and communication skills have not yet been integrated into cardiology education. Multiple online courses are available, including through my own organization, the Center to Advance Palliative Care (CAPC). Many cardiologists have free access to CAPC’s online courses through their member organizations.
Palliative care consultations can be helpful for complex decisions, refractory symptoms, family conflict and other challenging circumstances. Most large hospitals now have inpatient palliative care teams, while access to community-based palliative care is growing. Cardiologists can access palliative care expertise through their health systems, by contacting their patients’ health plans and case managers and by checking the Palliative Care Provider Directory at getpalliativecare.org.
Include palliative care activities in MIPS quality reporting
Through the Merit-based Incentive Payment System (MIPS), cardiology practices can select six quality metrics to contribute to their performance scores. Cardiology practices can focus their efforts to improve patients’ quality of life—and be compensated for doing so—by selecting quality measures such as advance care planning and pain management (both of which are MIPS measures worth additional bonus points). Successful implementation of these efforts will also raise MIPS performance scores by preventing unnecessary ED visits and readmissions, thus resulting in lower costs.
With their symptoms well managed and a full understanding of what to expect with the disease, patients can spend more time at home with their families and less time in the hospital and emergency department.
Diane E. Meier, MD, is the director of the Center to Advance Palliative Care, a nonprofit organization dedicated to increasing the availability of quality healthcare for all people living with a serious illness.
