
Medicare Tiptoes Around Modernization with New Codes for Virtual Check-ins & Remote Consults

As a result of new billing codes that went into effect this year via the 2019 Physician Fee Schedule Final Rule, physicians and qualified healthcare professionals (QHPs) can now be reimbursed for a few non-face-to-face (NFTF) services, including virtual patient encounters and remote interprofessional conversations with certain colleagues. The subtext, suggested speakers at the American College of Cardiology (ACC) Cardiovascular Summit in February, is that the Centers for Medicare & Medicaid Services is acknowledging that clinicians are caring for patients and conferring with one another differently than they did a decade ago—and that such interactions have value.
“What’s notable is that these new codes reimburse physicians for what they are already doing for free,” says Edward T.A. Fry, MD, chair of St. Vincent Health and Ascension Health CV Service Lines in Indianapolis.
While that’s a plus that could be heartening to clinicians and administrators alike, downsides come in the form of significant limitations and potentially burdensome requirements, particularly around patient consent.
Virtual patient encounters
The 2019 Final Rule’s two new HCPCS (Healthcare Common Procedure Coding System) codes for NFTF services are:
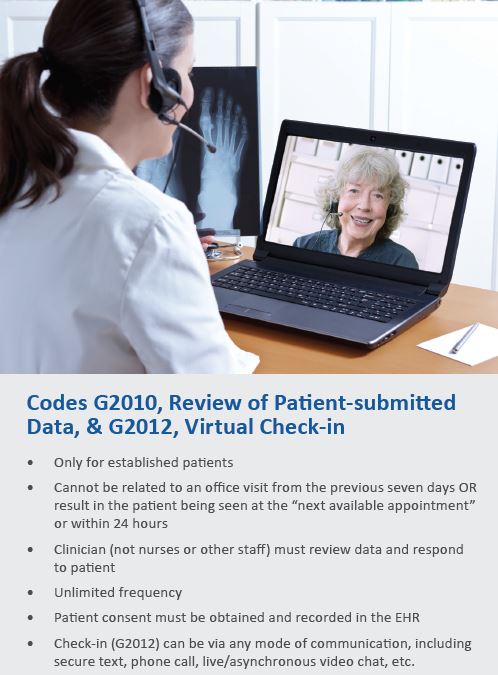
› G2010 for reviewing patient-submitted data, such as a video, picture or data from a consumer-level wearable (think: Apple Watch); and
› G2012 for five- to 10-minute, real-time “virtual check-ins” with patients, which include phone and other “synchronous, two-way audio interactions” with patients
Neither of the new codes is highly valued—approximately $13 and $15, respectively—but they do represent a leap forward by CMS, says Cathie Biga, RN, MSN, who co-directed the ACC’s summit and, as CEO of Cardiovascular Management of Illinois, manages nine practices in the Chicago area. Still, she adds, don’t use either code until you understand its limits. For starters, she warns, don’t confuse these codes with telehealth, which bills at a higher rate and has significant requirements.
Next, remember that G2012 is just for a check-in. As simple as it might sound, the task can’t be delegated to a nurse or other staff member. Only physicians and other QHPs qualify. Still, G2012 has promise for cardiologists who regularly see patients at remote clinics or whose patients face long commutes to the hospital, such as those coming in for transplant checks, says Linda Gates-Striby, CCS-P, ACS-CA, director of corporate compliance at St. Vincent Medical Group in Indianapolis. “It’s also a way to check in with more local patients who truly have extreme difficulty getting out and about.”
Getting reimbursed for NFTF encounters sounds good, even long overdue, but there’s a catch. When Gates-Striby first told clinicians about G2010 and G2012, they were excited, but their enthusiasm waned as they learned that both codes have a copayment and, therefore, require patient consent and documentation in the electronic health record each time the service will be billed.
This requirement could be an insurmountable hurdle for some practices, predicts Biga. Of course, it needs to be clear to patients that there will be a charge, she says, but the mechanics of obtaining consent will be a deterrent for many practices. “I don't think [we’re] going to be using this much,” she adds.
Interprofessional remote consultation
Another set of possibly revenue-enhancing codes arrived in the form of new Current Procedural Terminology (CPT) codes that cover remote interactions with referring, requesting or treating physicians or QHPs.
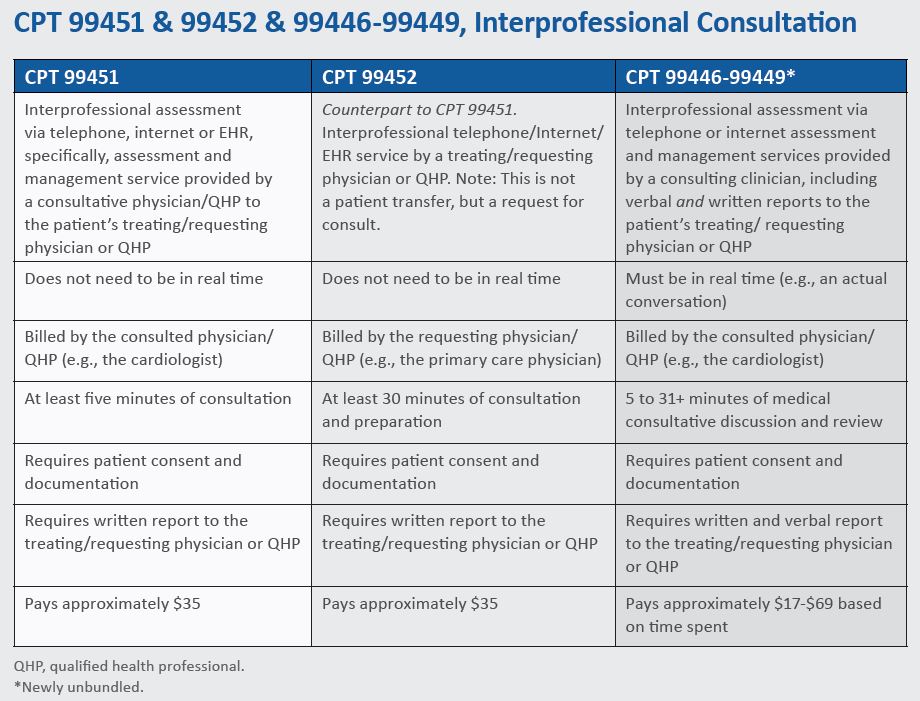
CPT 99451 and 99452 are for “interprofessional assessment” via telephone, internet or EHR, with the former code used by a consultative clinician to the patient’s treating/requesting clinician and the latter by the requesting clinician. CPT codes 99446-99449, which were recently unbundled, cover telephone or internet assessment and management services provided by a consulting clinician, including verbal and written reports to the patient’s requesting physician or QHP. “It would be like the PCP and the cardiologists having a conversation, [such as] ‘Now, how can we manage the atrial fibrillation or the heart failure or whatever?’” Gates-Striby explains.
You might think these codes would result in easy money because physicians consult one another frequently, and often remotely, says Gates-Striby. But here again, a patient consent requirement creates an obstacle. In fact, it could be a bigger challenge than for G2010 and G2012 because interprofessional consultations can—and often do—occur without any patient contact. “Explaining it to the patient is going to require some strategizing,” she says. “It can be an awkward conversation.”
Reimbursement for what you already do
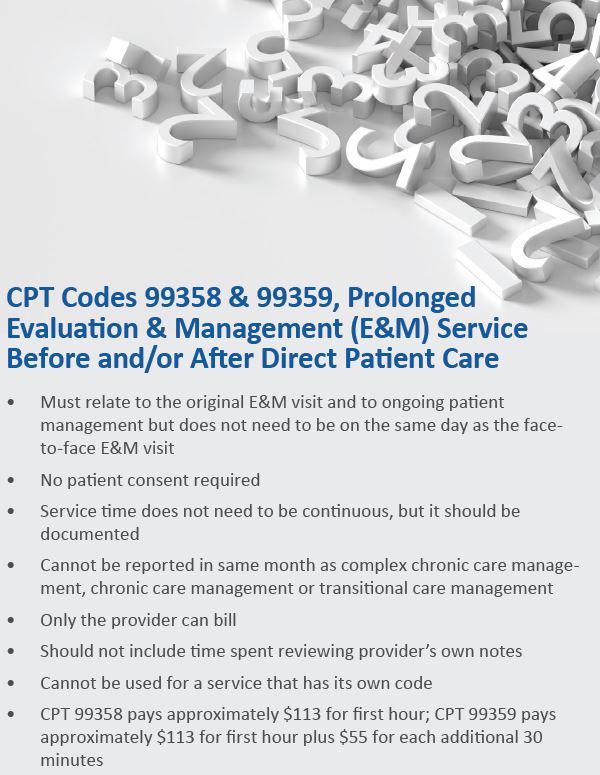
Amidst mixed messages of new money that comes with significant challenges is good news that isn’t really news at all. In 2018, CMS activated CPT codes 99358 and 99359—two codes that are separately billable and reimbursable for NFTF prolonged service for evaluation and management (E&M) service before and/or after direct patient care, with “prolonged” defined as “beyond the usual time.”
These codes provide better reimbursement rates than the 2019 NFTF codes discussed above, do not require patient consent and reimburse physicians and QHPs for tasks they are already doing. Moreover, Gates-Striby reports, almost every payer (commercial and public) is reimbursing for this pair of codes.
The activities don’t even need to be on the same day, she explains. A cardiologist could spend 20 minutes the night before a visit reviewing a patient’s lab work and then, a week after the E/M visit, look at some imaging studies. As long as the activities tie into the ongoing management of the patient—but are outside the scope of the face-to-face visit itself—it’s billable. There are a few exceptions; these codes—
› cannot be reported during the same month as complex chronic care management, chronic care management or transitional care management
› cannot include time spent in reviewing the physician’s or QHP’s own notes
› cannot be used for a service that has its own code
They are “the most efficient, easiest to use, best codes,” especially for cardiology, says Biga. “They don’t have all the goofy rules of the new G codes and some of the interprofessional codes. That’s really important.”
What’s odd, Biga says, is that she hasn’t seen many practices using these year-old codes even though they “truly represent new money.” Gates-Striby reports the same thing, although the physicians she works with are enthusiastic and attendees at the ACC Cardiovascular Summit were quick to snap photos of her slides on this topic.
If the codes have penetrated anywhere, it’s among proceduralists who work in subspecialized areas such as pediatric cardiology, structural heart disease and complex coronary interventions, especially physicians who treat chronic total occlusions (CTOs), says Fry.
“One of our interventionalists has built it into a CTO,” adds Gates-Striby. “[CTO procedures] take tons of planning. Anytime he’s looking at info for that procedure, he records the time—on a paper form.”
Yes, paper, because they haven’t figured out how to make their EHR accommodate the documentation needs associated with CPT codes 99358 and 99359.
No doubt, the workflow for these codes is challenging and can be a hassle—even though there is no consent requirement. Practices need to develop a system to ensure the additional time spent on complex patients is documented accurately, emphasizes Gates-Striby. Her team created a form for physicians to document their activities and time spent. A staff member scans each completed form into the EHR, where it’s linked to the in-person encounter.
It’s a start
With the NFTF and prolonged service codes, Medicare basically acknowledged that time is a physician’s greatest commodity, and it’s beginning to reflect that in how it pays, says Gates-Striby. But, especially with the new 2019 codes, much needs to be worked out to make the new money worth the challenges of earning it.
Considering the complexity of the rules, CVB had to ask, “Is there really any new money on the table?” “Yes, this is all new money,” Biga replied. “But what does it cost to get that money?”
As always, Cardiovascular Business has made every effort to confirm that the information in this story is accurate and
current; however, it should not replace the expertise of your coding staff. Codes and requirements change so always be sure your model fits the requirements.