
Choosing left radial access in the cath lab helps cardiologists limit radiation exposure
Using a left radial artery (LRA) approach in the cath lab is associated with significantly less radiation exposure for interventional cardiologists than a hyper-adducted right radial artery (HARRA) approach, according to new data published in Circulation: Cardiovascular Interventions.[1]
“Cardiac catheterization from the radial approach increases the safety profile for patients and decreases institutional costs,” wrote first author Richard Casazza, MAS, RT, a cath lab technologist with Maimonides Medical Center in Brooklyn, New York, and colleagues. “Data regarding operator radiation exposure when using left or right radial artery approaches are mixed.”
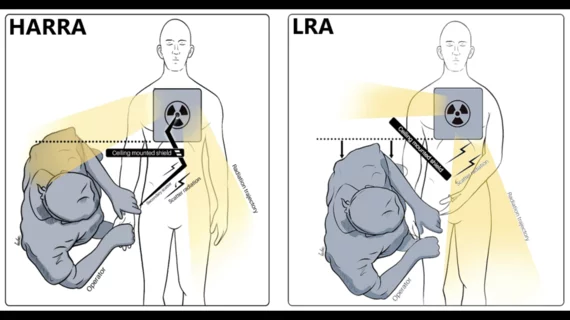
To learn more, Casazza et al. performed a single-center randomized controlled trial focused comparing the LRA and HARRA approaches. Real-time radiation dosimeters were placed on the thorax, abdomen, left and right eye of each operator during 534 diagnostic catheterization procedures. Procedures were randomized to be performed using either the LRA or HARRA approach.
Overall, cumulative radiation measurements as measured in microsieverts [μSv] were consistently lower for operations that utilized the LRA approach. This included lower mean cumulative totals in the thorax (9.6 μSv for LRA vs. 12.27 μSv for HARRA), the abdomen (27.46 μSv for LRA vs. 36.56 μSv for HARRA), the left eye (2.65 μSv for LRA vs. 3.77 μSv for HARRA) and the right eye (1.13 μSv for LRA vs. 1.44 μSv for HARRA).
Normalized radiation measurements were also lower for all four parts of the body, and the LRA approach had a lower subclavian tortuosity (15.6%) than the HARRA approach (32.5%).
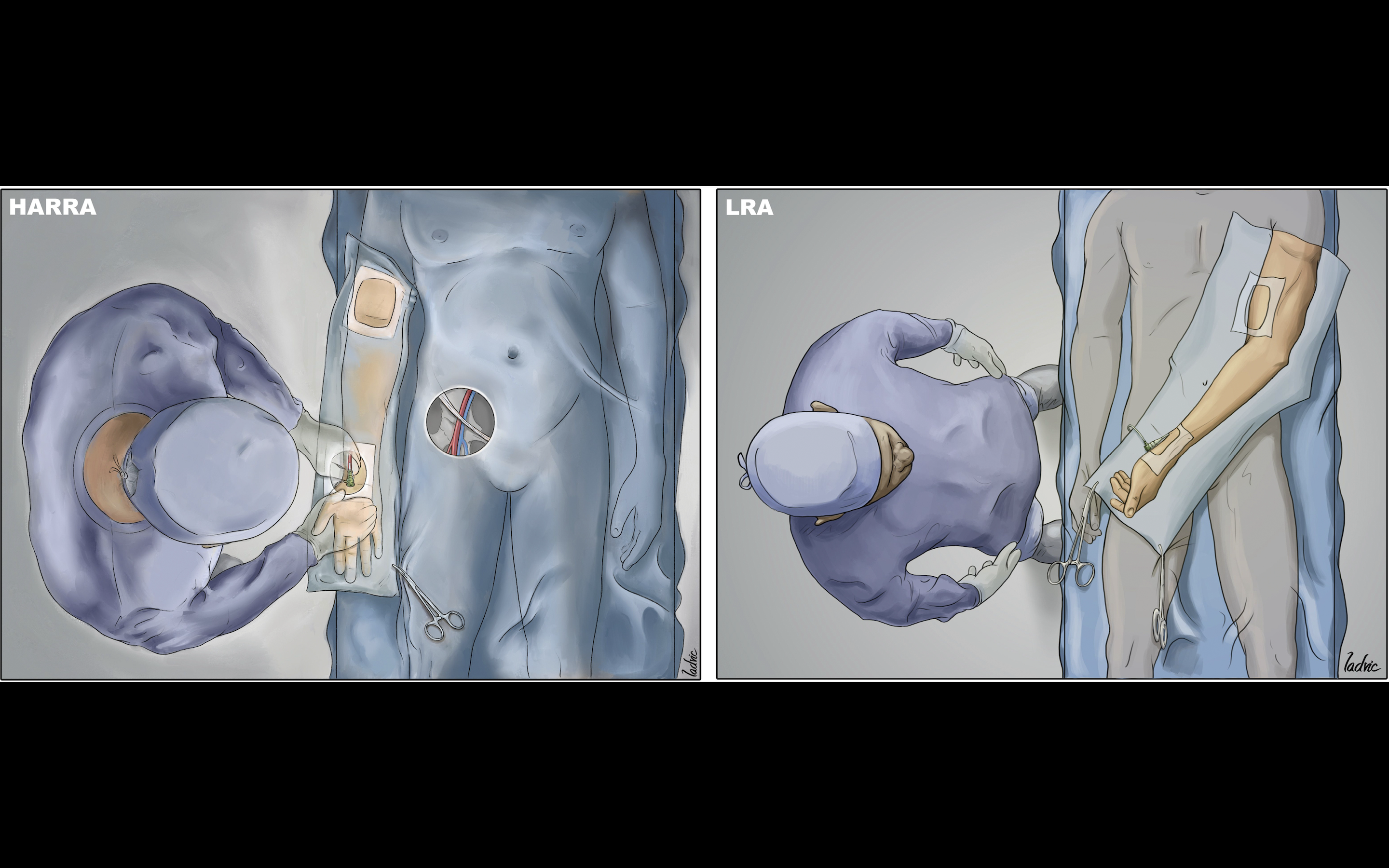
Image courtesy of Casazza et al. and Circulation: Cardiovascular Interventions.
“These data should encourage the use of the LRA as the primary access site for cardiac catheterization,” the authors wrote. “This paradigm shift can reduce occupational radiation exposure for interventional cardiologists. Currently, the right radial artery is the most utilized access site due to standard cardiac catheterization laboratory configurations and ergonomic considerations; however, proper setup for the LRA can address potential ergonomic concerns.”
The group also highlighted the role patient anatomy can play when it comes to radiation exposure.
“Previous studies have attributed radiation reductions when using the LRA to a higher frequency of right subclavian tortuosity compared with left subclavian tortuosity,” they wrote. “Indeed, in the present study, the LRA group had a lower proportion of subclavian tortuosity than the HARRA group.”
Casazza and colleagues called for more research into this topic, noting that it remains unknown how different factors such as operator experience may impact overall levels of radiation exposure.
Click here for the full analysis.

Michael has more than 18 years of experience as a professional writer and editor. He has written at length about cardiology, radiology, artificial intelligence and other key healthcare topics.