
Get Ready: CT-guided PCI Is Coming to a Cath Lab Near You

Change is on the horizon for cath labs all over the world as more and more interventional cardiologists are starting to use coronary CT angiography to plan and guide percutaneous coronary intervention (PCI) procedures. Patients, physicians, catheterization labs and healthcare systems all stand to gain from an evolution that is “the way of the future,” says Carlos Collet, MD, PhD, co-director of the catheterization lab OLV Hospitals in Aalst, Belgium.
“CT-guided PCI is changing how we plan and guide coronary interventions, providing a more precise and efficient method to diagnose and treat heart disease,” Collet explains. “It’s already making a big impact in our lab, and that influence will only grow as time goes on.”
Collet and his team, among others, are leading the charge in both treating patients and educating interventionalists and cardiologists across the globe. He also played a key role in the development of an expert consensus document on the topic for the Society of Cardiovascular Computed Tomography in November 2022.[1]
As the consensus document notes, coronary CT can add significant value in a number of areas, shining where other modalities struggle. Consider, for instance, its detailed plaque assessments, which detail the plaque’s extension, volume and composition. CT exams also can predict the procedural success of chronic total occlusion PCI procedures, identify lesions that may need additional treatment and help heart teams make final treatment decisions when considering patients with complex or multivessel coronary artery disease (CAD).
Offering deeper, more visual and intuitive information to plan and guide PCI procedures will enable better outcomes for CAD patients who need percutaneous revascularization at lower costs, Collet predicts. Implementation of CT-guided PCI is also expected to help providers optimize resources, staffing and cath lab utilization.
Coronary CT’s move into PCI workflows builds on the modality’s success in noninvasively detecting and excluding CAD, a use that has picked up momentum in recent years thanks in part to recommendations published by the European Society of Cardiology in 2019 and American Heart Association and American College of Cardiology (ACC) in 2021.[2,3] Because coronary CT can effectively rule out significant CAD, it helps limit the use of invasive coronary angiography (ICA) when it is not clinically necessary.

“CT-guided PCI is changing how we plan and guide coronary interventions, providing a more precise and efficient method to diagnose and treat heart disease."
- Carlos Collet, MD, PhD, Co-director of the Catheterization Lab, OLV Hospitals, Aalst, Belgium
Even when it is needed, ICA has a key weakness: it can only assess the vessel’s lumen, not the plaque itself. This limitation puts the operator at a significant disadvantage.
“You cannot see if the plaque is lipid or calcium on ICA and you cannot see where it begins or ends,” Collet notes. “So we have been implanting stents all these years without this helpful information. We make our views in the cath lab and then have just 10 or 20 seconds to decide what we are going to do next.”
This is why PCI needs guidance. CT-guided PCI provides significant value in the cath lab—and could make interventional cardiologists completely rethink the way they approach revascularization. Most importantly, this information is readily available before the procedure, allowing specialists to plan before stepping into the cath lab.
“While CT has been an excellent tool to diagnose, it also is very useful for guiding revascularization procedures,” Collet says. “Being aware of the disease that you're about to treat offers you the possibility to not only be prepared for what you're going to do, but also all the things that you need to do to make that PCI the best you can. This is where the field is going.”
The continued evolution of CT
Improving CT guidance begins with enhancing CT technology. If coronary CT had not evolved to effectively visualize a patient’s plaque, for instance, CT-guided PCI would have never even entered the conversation. The modality has seen other improvements in recent years that have also helped make this new technique a reality.
For example, CT exams are associated with much less radiation exposure now than they were in the past. One recent analysis found that the median dose-length product of a coronary CT dipped from 885 mGy cm in 2007 to 195 mGy cm in 2017.[4] This alone could play an important role in making interventional cardiologists, cath lab managers and other stakeholders more likely to pursue a treatment that revolves around coronary CT.
In addition, physicians can now utilize a physiologic simulation technique that models coronary flow from routine coronary CT angiography. The CT-derived fractional flow reserve (FFR-CT) technology identifies exactly where reduced blood flow exists and assesses the severity of any blockages. FFR-CT results can be added to a patient’s coronary CT results to provide more data on patient disease and treatment options. Also, the FFR-CT technology simulates PCI, known as virtual PCI, in a way that predicts how different treatments may affect the target vessel.
FFR-CT also can determine whether a patient’s CAD is diffuse or focal. “This is important, because those are two very different things,” Collet says. “Patients with focal disease can be treated with stents, but stents are not always a good idea when the patient has diffused disease.”
Planning ahead
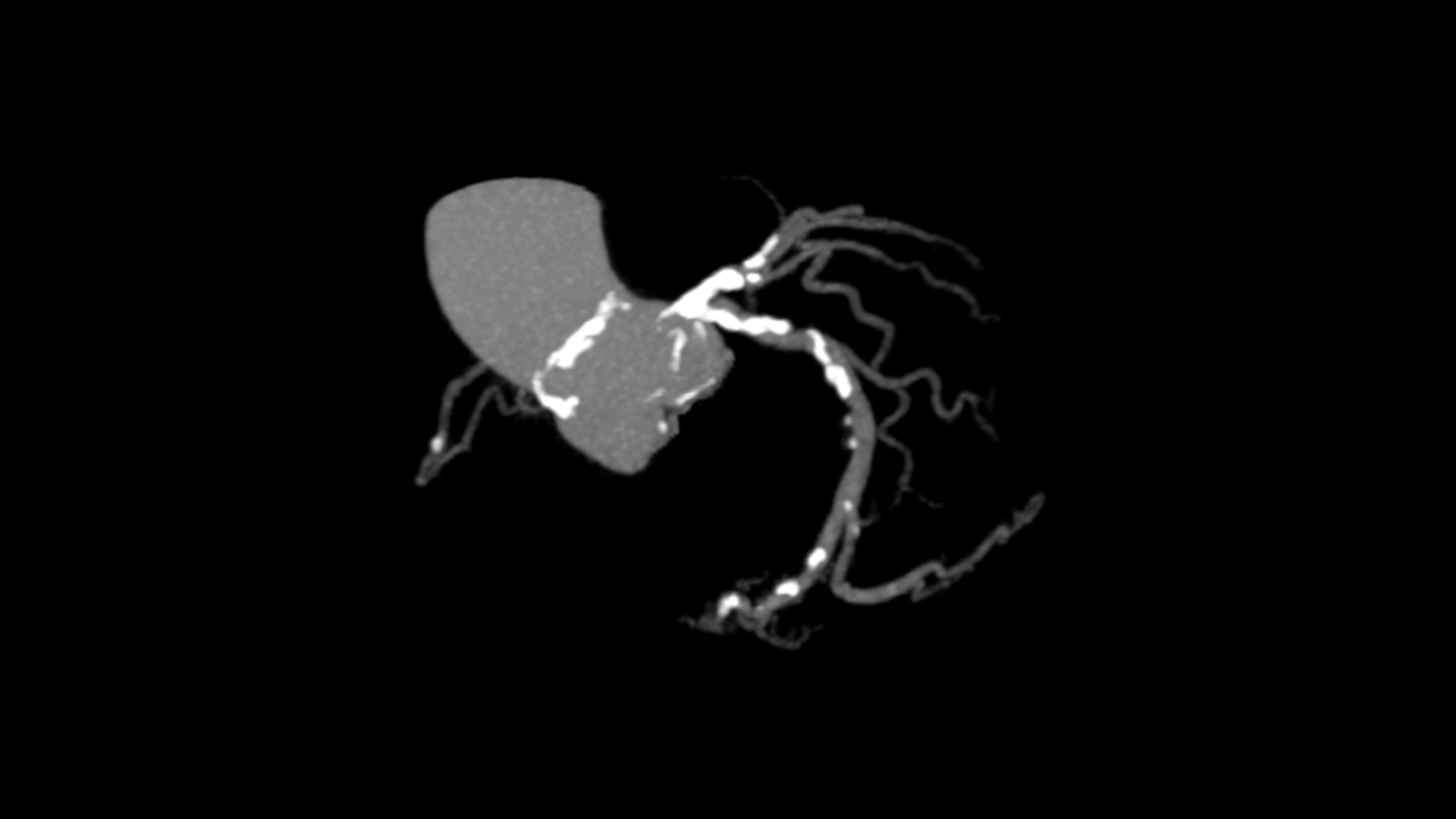
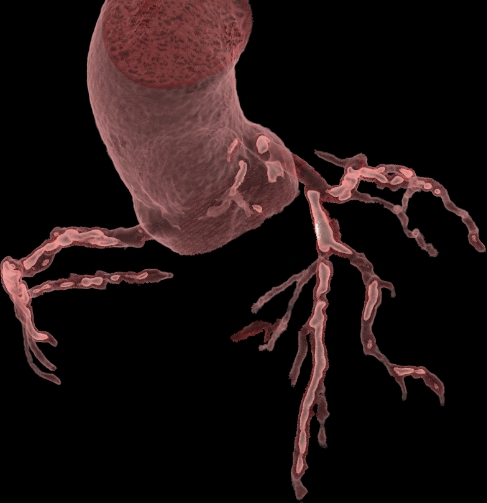
Coronary CT’s ability to visualize the patient’s plaque helps operators plan for a procedure in advance. Instead of “going in blind” as is most often the case, they can study the converted 3D images—which are color-coded so blood appears red, and calcium appears white—so that they know exactly what to expect.
“It helps the cardiologist know if it will be a straightforward case, one that might be finished in just 10 minutes or so, or if it’s going to be much more complicated,” Collet says. “Maybe there’s a ton of calcium that will need to be treated, turning it into a two- or three-hour procedure.”
Other key details that can now be planned out in advance are the size and type of catheter the operator will need. This saves time, money and also limits pain and discomfort for the patient. Stents also can be selected in advance, and if any other specific tools are going to be required—like for an especially severe lesion—the team can have those tools all lined up and ready to go.
“This may seem like a small thing, but it helps to have everyone already be on the same page before the procedure has even started,” Collet says.

Planning ahead impacts more than just the individual cardiologist. It also helps cath labs schedule patients and ensures the right operator is being assigned to the right case.
“We classify each patient according to the complexity of the disease and the treatment that will be required,” Collet says. “And then we use that information when deciding how much time to allocate for each PCI. It makes the cath lab more efficient, which makes the entire health system more efficient.”
A downstream benefit to this upgrade in efficiency is being able to treat more patients per cath lab per day. This is good news for CV service line managers and directors as well as executives keeping a close eye on the bottom line.
Collet also says that he has seen very few downsides to the implementation of CT-guided PCI.
“The only real issues we have encountered are the same limitations that are true for all coronary CT examinations,” he says. “Patients with stents can be difficult to image, for example, and so can patients with arrhythmias such as atrial fibrillation. Obese patients can pose logistical problems. These are just the limitations of CT as a modality. Fortunately, we have other modalities that we can use when such a situation arises.”
Training sessions help interventional cardiologists get to know the technology
Collet notes that interventional cardiologists have a history of shying away from new technologies they do not fully understand. Intravascular imaging-guided PCI, for example, has been associated with strong clinical outcomes, but adoption remains quite low.
“The main problem is the interpretation of the information,” he says. “It has a steep learning curve, and when you do something that confuses you, you don’t want to do it again. You lose confidence. You don’t know how to react to the information, so it loses value.”
To help ensure the same thing does not happen with CT-guided PCI, Collet and his colleagues at OLV-Aalst are offering two-day courses specifically designed to help teach interventional cardiologists how to properly interpret coronary CT exams and get the most benefit out of this promising technique. In addition to hands-on simulator training and live cases, the courses also allow specialists to network with one another, work together and gain a better understanding of how CT-guided PCI can improve patient care.
“CT is a diagnostic tool primarily used by radiologists and imagers, so the typical interventional cardiologist does not know how to read these results,” Collet says. “And even though we are now working with images that have been conveniently color coded, cardiologists still need to understand what the images mean. That was the primary reason we started offering this dedicated course.”
“In the future, CT will become a core competency for interventional cardiologists. Multiple scientific guidelines recommending coronary CT as a first-line treatment is only going to help that even more."
- Carlos Collet, MD, PhD, Co-director of the Catheterization Lab, OLV Hospitals, Aalst, Belgium
General cardiologists are starting to take the course, too. Collet says that multiple colleagues have told him that learning more about CT-guided PCI has changed the way they think about these procedures.
“One of my colleagues flew in from New York for the course last year, and then I just saw him again a few days ago,” he says. “He told me that this has completely changed how he prepares for a PCI, that now he loves to open the CT because he really recognizes what he is looking at. It has made him much more prepared before he even walks into the cath lab. This shows us that, yes, CT-guided PCI can be really impactful.”
Ongoing research into the benefits of CT-guided PCI
There is still plenty more to come for this evolving technique. Collet, a passionate researcher, has co-authored dozens of clinical studies on CAD, PCI and other interventional topics over the years, including one for JACC: Cardiovascular Imaging focused on the implementation of coronary CT in cath labs[5]. He is currently working on the Precise Procedural and PCI Plan (P4) trial, which will compare the safety and effectiveness of CT-guided PCI compared with intravascular ultrasound (IVUS)-guided PCI in a cohort of 1,000 patients with stable CAD and significant obstructions.
While the trial’s primary clinical endpoint is focused on major adverse cardiovascular events—including cardiovascular death, myocardial infraction and repeat revascularization—secondary endpoints will examine procedural time, resource utilizations and healthcare costs. Collet is one of the study’s principal investigators; the other is Daniele Andreini, MD, PhD, a cardiologist and radiologist at Milan University in Italy.
The P4 trial is examining economics and efficiency as well. Secondary findings will look at in-hospital resource utilization during the intervention between coronary CT- and IVUS-guided PCI strategies. Procedure duration and all costs related to the patient’s hospitalization will be examined at length, as will radiation dose and contrast volume.
The study started enrolling patients in March 2022, with about 120 patients included to date. Collet and Andreini hope to have some initial data in late 2026.
“In cardiology, it is very important to have clinical evidence, and we’re generating more evidence with every single patient,” Collet adds. “Each case is a new learning experience. We hope that our research, in addition to the training courses, can help show interventional cardiologists all over the world that CT-guided PCI is a powerful tool that can make a big impact on patient care.”
Collectively, he adds, the team behind the P4 trial has hypothesized that CT-guided PCI will be linked to similar outcomes and cost savings compared to intravascular imaging-guided PCI.
“Because of the prediction of what is the optimal treatment strategy to obtain a perfect result, the patients treated with CT-guided PCI may feel better than other patients,” he says.
Looking to the future
Collet says he anticipates “an explosion” in CT-guided PCI coming to interventional cardiology sooner than later.
“In the future, CT will become a core competency for interventional cardiologists,” he says. “Multiple scientific guidelines recommending coronary CT as a first-line treatment is only going to help that even more. This technology is here now, yes, but it will become the standard of care in another 10 years.”
Collet also is quick to emphasize that IVUS, OCT and other imaging modalities will still be of great value to PCI operators who want to use them.
“We are not pitching this as a substitute for other modalities,” he says. “Those other technologies will remain. They still provide added value. But coronary CT is a perfect complement to angiography that can deliver information in a way that was not feasible before. It will become a core competency of interventional cardiologists. It’s a resource we are very lucky to have in our cath labs.”
References:
1. Daniele Andreini, Carlos Collet, Jonathon Leipsic, et al. Pre-procedural planning of coronary revascularization by cardiac computed tomography: An expert consensus document of the Society of Cardiovascular Computed Tomography. J Cardiovasc Comput Tomogr. 2022 Nov-Dec;16(6):558-572. https://doi.org/10.1016/j.jcct.2022.08.003.
2. Juhani Knuuti, William Wijns, Antti Saraste, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes: The Task Force for the diagnosis and management of chronic coronary syndromes of the European Society of Cardiology (ESC). European Heart Journal, Volume 41, Issue 3, 14 January 2020, Pages 407–477, https://doi.org/10.1093/eurheartj/ehz425.
3. Martha Gulati, Phillip D. Levy, Debabrata Mukherjee, et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation, 2021;144:e368–e454, https://doi.org/10.1161/CIR.0000000000001029.
4. Stocker TJ, et al. Reduction in radiation exposure in cardiovascular computed tomography imaging: results from the Prospective Multicenter Registry on RadiaTion Dose Estimates of Cardiac CT AngIOgraphy IN Daily Practice in 2017 (PROTECTION VI). Eur Heart J. 2018;39(41):3715-3723, https://doi.org/10.1093/eurheartj/ehy546.
5. Carlos Collet MD, PhD, Jeroen Sonck MD, Jonathon Leipsic MD, et al. Implementing Coronary Computed Tomography Angiography in the Catheterization Laboratory. J Am Coll Cardiol Img. 2021 Sep, 14 (9) 1846–1855. https://doi.org/10.1016/j.jcmg.2020.07.048.

Michael has more than 18 years of experience as a professional writer and editor. He has written at length about cardiology, radiology, artificial intelligence and other key healthcare topics.