
Cardiologists are first in world to use new cooling device to terminate AFib during surgery

Cooling the oblique sinus of the heart may be a safe, effective way to quickly terminate atrial fibrillation (AFib) that develops during a cardiac surgery, according to a new first-in-human study published in Heart Rhythm O2.
Patients often develop AFib during cardiac surgery, leading to longer hospital stays, additional healthcare costs and a significantly higher risk of mortality. The study’s authors explored a new way to potentially terminate perioperative AFib: using a small device to cool the oblique sinus in a way that could potentially be done without anesthesia.
“We have previously demonstrated the effectiveness of cooling the oblique sinus to terminate AFib in animal models,” wrote corresponding author Paul A. Friedman, MD, a cardiac electrophysiologist with Mayo Clinic, and colleagues. “However, humans undergoing cardiac surgery often have common comorbidities, including advanced age, hypertension, diabetes and concomitant structural and fibrotic changes, which may impact therapy effectiveness. To determine whether cooling would be effective for the termination of AFib in humans, we performed a pilot feasibility study.”
Friedman et al. test the technique out on a total of four patients with a mean age of 69.3 years old. All four patients were women with a history of paroxysmal AFib and underwent clinically indicated cardiac surgery, whether it was coronary artery bypass grafting, an aortic valve replacement or mitral valve surgery. AFib was induced in these patients via rapid atrial pacing; clinicians allowed it to persist for 30 seconds before working to terminate it. If the AFib did not sustain for long enough, the group tried again for up to three attempts total.
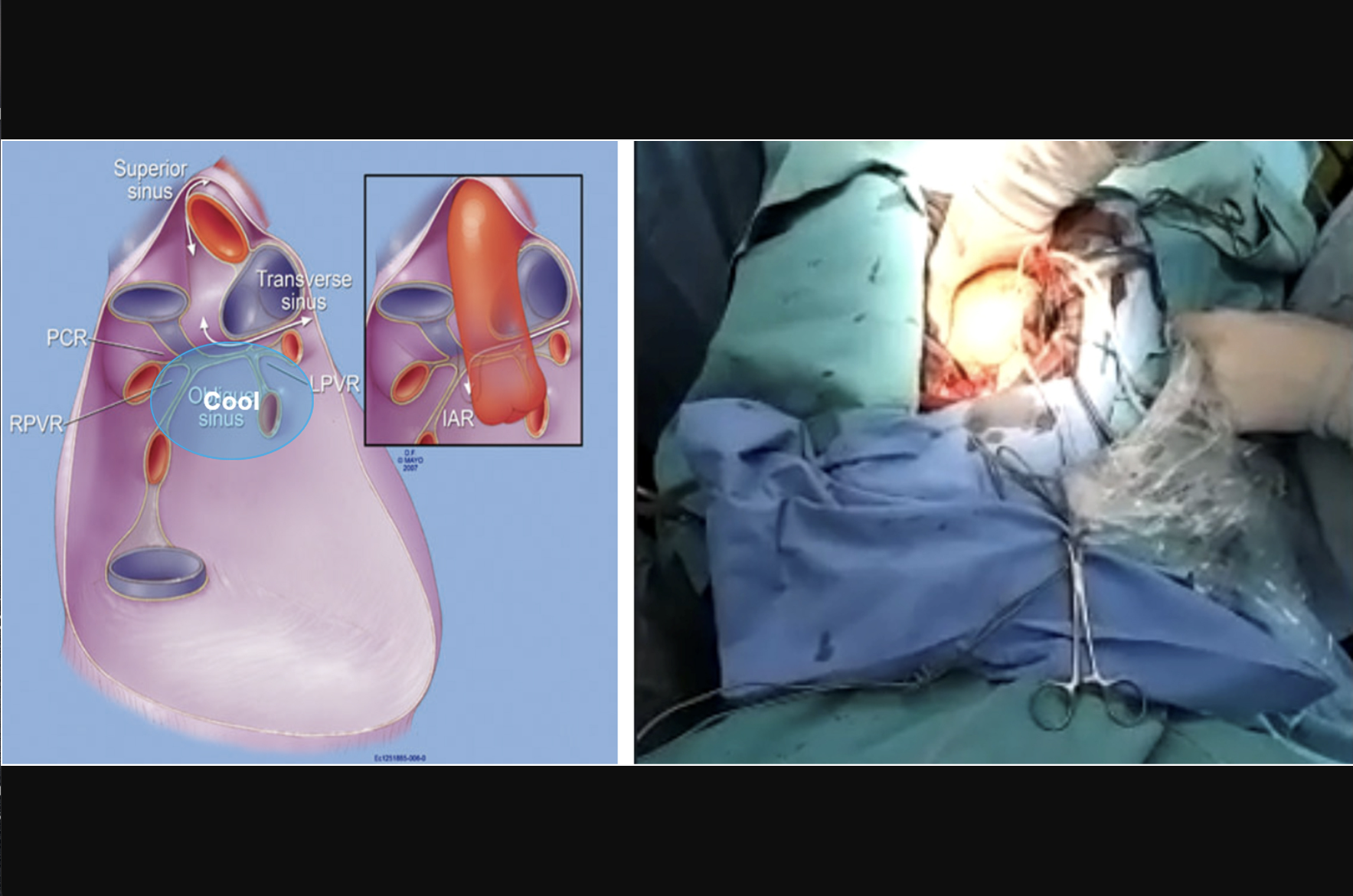
(Left) Anatomical depiction of the oblique sinus. The pericardium is shown with the anterior section and heart removed. The region to which cooling was applied is shown with the blue oval labelled “Cool.” (Right) Surgical placement of the device in the oblique sinus in one of the patients in the study. Note that the right panel is a captured image from a live, remote transmission, accounting for blurriness. Images and caption courtesy of Heart Rhythm O2 and the Heart Rhythm Society.
The cooling device used for these procedures was approximately 1 inch x 1 inch. It was attached to a bedside chiller that cooled saline and sent it to the device. The temperature was monitored at all times through electrical connectors.
Overall, eight AFib episodes were induced in the four patients. Five of those eight episodes were terminated with cooling, and the average time to termination—after the initial 30 seconds—was 21 seconds. The temperature never dropped below 5 degrees Celsius/41 degrees Fahrenheit.
There were three cases where the AFib was not successfully terminated. In one of those cases, the patient actually developed bradycardia and ventricular fibrillation, so it was stopped immediately and addressed by the clinicians. No clinical complications were reported.
The group also emphasized that the clinically indicated surgeries were all performed without any complications related to this research.
“In this first-ever human feasibility study, we found that cooling in the oblique sinus to terminate perioperative AFib is feasible and appears safe,” the authors wrote. “Specifically, we found that lowering the average temperature below 13 degrees Celsius/55.4 degrees Fahrenheit successfully terminated AFib, most commonly in under 30 seconds, and in all cases in under one minute. In no cases did the temperature drop below 5 degrees Celsius/41 degrees Fahrenheit, and there were no findings to suggest any temperature-related injury. Importantly, 13 degrees Celsius/55.4 degrees Fahrenheit is a temperature at which no intracellular ice crystals or long-term damage to cardiomyocytes or surrounding tissues occur.”
The group added that its long-term goal is to “effectively treat AFib painlessly.” By using these cool temperatures, they hope they can use this advanced technology to make that goal a reality.
“As this was a very early feasibility study, the number of observations is small, and there is no control group,” the authors concluded. “A larger study with control individuals is necessary to confirm safety, efficacy, and impact on clinical outcomes.”
This study was funded by Michigan-based MediCool Technologies, the company working on this cooling technology. One co-author was a MediCool employee. In addition, two co-authors—Friedman and Samuel Asirvatham, MD—are co-inventors of the technology.
Click here to read the full study in Heart Rhythm O2, an open-access journal from the Heart Rhythm Society.

Michael has more than 19 years of experience as a professional writer and editor. He has written at length about cardiology, radiology, artificial intelligence and other key healthcare topics.