
How expert guidelines have influenced TAVR vs. SAVR decisions
Surgical aortic valve replacement (SAVR) utilization has declined since the introduction of transcatheter aortic valve replacement (TAVR). However, according to new data presented at the American Association for Thoracic Surgery (AATS) 106th Annual Meeting in Chicago, SAVR started to regain momentum around the time the 2020 American College of Cardiology (ACC)/American Heart Association (AHA) guidelines on valvular heart disease were released.
Sean Nguyen, MD, a researcher at the University of Minnesota, presented these data at the AATS conference.
"These findings suggest room to expand the use of SAVR in select patients under 80 and support the need for long-term outcomes of guideline-based valvular care," he said.
The study also found that inpatient mortality and major adverse cardiac events (MACE) after SAVR remain unchanged after guideline recommendations were implemented.
The 2020 guideline included recommendations for when to use SAVR vs. TAVR based on a heart team's decision that focuses more on age, life expectancy and valve durability and less on traditional surgical risk scores. SAVR is recommended for patients younger than 65 with a life expectancy of more than 20 years. SAVR, meanwhile, was no longer recommended in patients age 80 and older with a life expectancy of less than 10 years.
On the other hand, there is a gray area for the ages of 65 to 80 where TAVR or SAVR may be the best option. That's where shared decision-making plays a major role.
Nguyen said this gray area also offers possible growth for SAVR under the argument that younger patients should have surgery first so that later valve replacements when a patient is older and more frail can be done using minimally invasive TAVR.
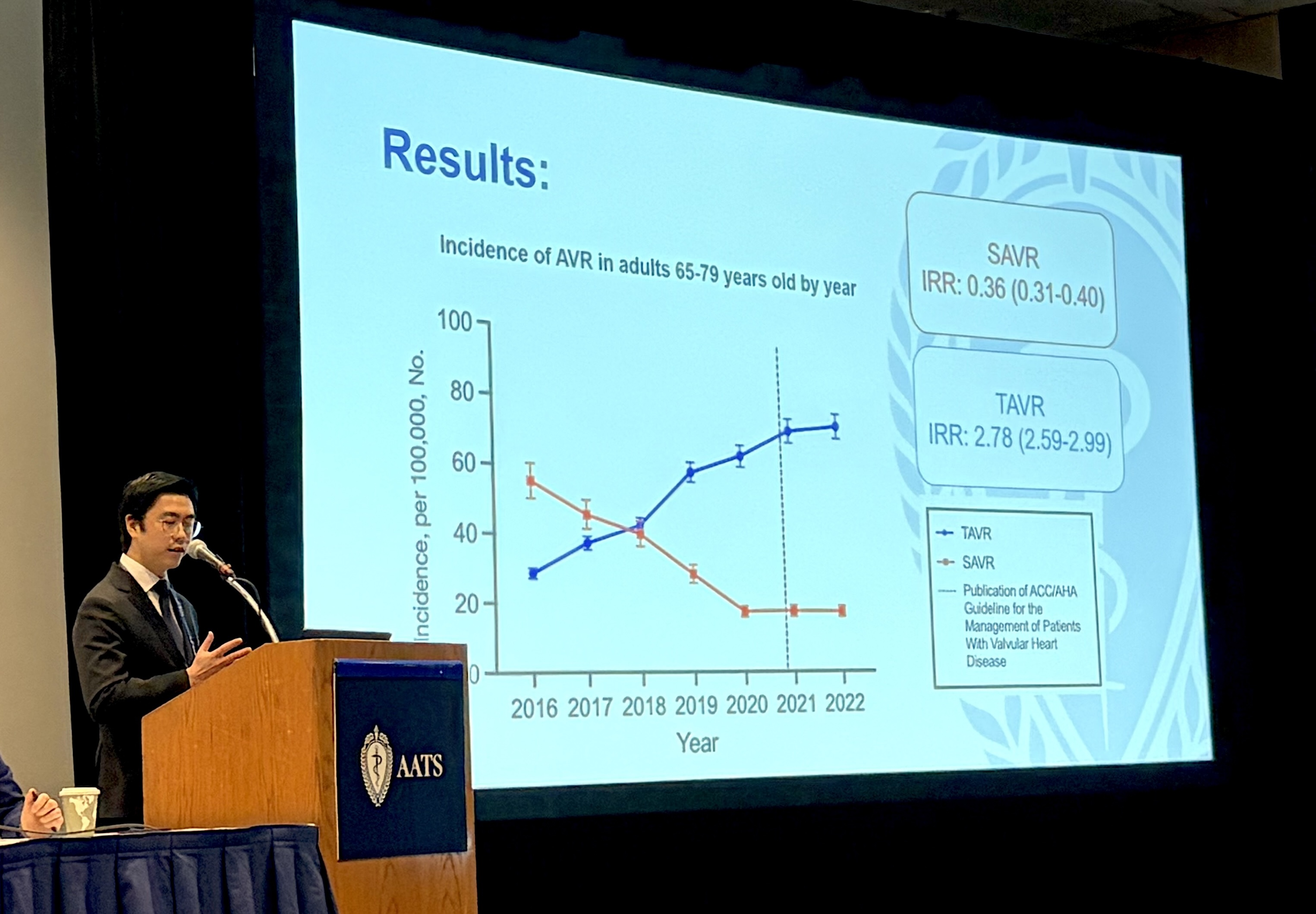
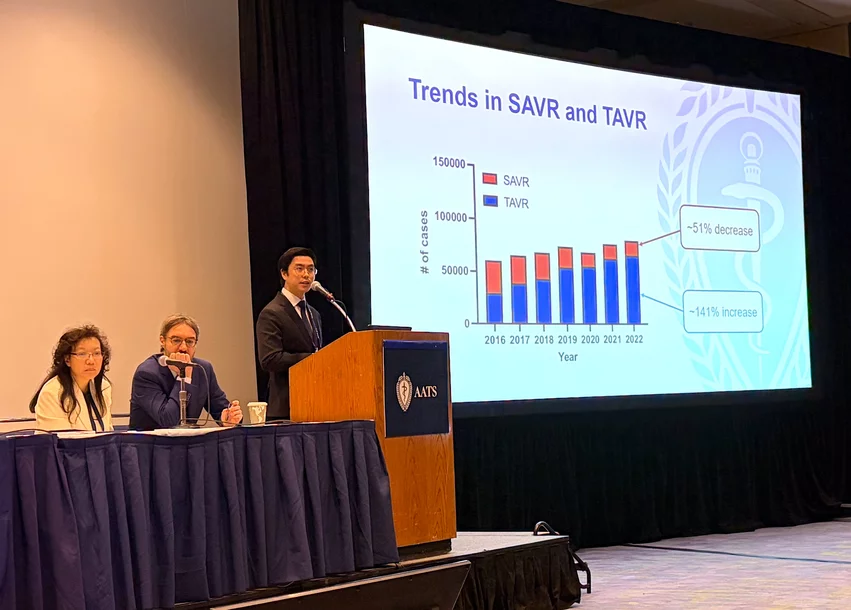
The study showed that while TAVR continued to increase in volume through 2022, SAVR volumes stabilized and plateaued starting in 2020.
Nguyen presented data on the changes in the age of patients receiving TAVR and SAVR. Aortic valve replacement volumes have really started to rise in patients age 50 and older, with the majority of procedures getting replacements between ages 65 and 85. Pre-guideline TAVR and SAVR patient volumes intersected at about age 70, and SAVR was still being used in a sizable number of patients over age 85.
But following the guideline publication, the intersection of volumes moved to about age 64, as TAVR picked up more of these younger patients. SAVR numbers also noticeably dropped for all patient age groups after age 64, and SAVR numbers completely drop off around age 85 as TAVR took over in all of these older, high-risk patients.
The data also show that while TAVR continued to increase in volume through 2022, SAVR volume stabilized and plateaued in 2020, prior to the publication of the guidelines late in the year.
To look at the impact of the guideline change for this study, researchers pulled data between 2016-2022 from the National Inpatient Sample, the largest publicly available all-payer, inpatient hospital database. It includes 97% of the U.S. population.

Dave Fornell has covered healthcare for more than 17 years, with a focus in cardiology and radiology. Fornell is a 5-time winner of a Jesse H. Neal Award, the most prestigious editorial honors in the field of specialized journalism. The wins included best technical content, best use of social media and best COVID-19 coverage. Fornell was also a three-time Neal finalist for best range of work by a single author. He produces more than 100 editorial videos each year, most of them interviews with key opinion leaders in medicine. He also writes technical articles, covers key trends, conducts video hospital site visits, and is very involved with social media. E-mail: [email protected]