
Intravascular lithotripsy helps address the challenges of transvenous lead extraction
Intravascular lithotripsy (IVL) can provide significant value during transvenous lead extraction (TLE) procedures by identifying dense calcifications, according to new research published in JACC: Clinical Electrophysiology.[1]
“Despite the fact that TLE procedures have been performed for six decades, little progress has been made in targeting one of the most common confounding aspects of these procedures: the presence of dense calcifications encasing the leads within the vasculature,” wrote co-authors Christopher A. Latanich, MD, and John A. Anderson, DO, with the Heart and Vascular Institute in Duluth, Minnesota. “When present, this can significantly increase the difficulty, complexity, and risk of an extraction procedure.”
The two authors aimed to find out if IVL, a relatively new technology first developed by Shockwave Medical, could help manage these dense calcifications during TLE procedures. IVL involves attacking calcified lesions with acoustic pressure waves delivered by a catheter. It is currently approved by the U.S. Food and Drug Administration for the treatment of peripheral arterial disease and coronary artery disease.
To examine IVL’s potential, the two researchers examined data from 65 patients who underwent TLE and explantation procedures from October 2019 to April 2023. While all TLE procedures from October 2019 to June 2022 used conventional extraction techniques, procedures from July 2022 to April 2023 added the use of IVL technology.
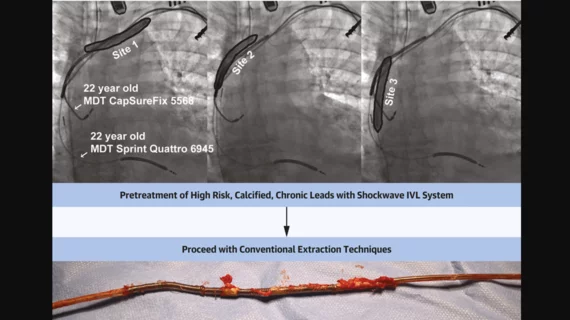
Before each procedure, cardiac CT exams were performed to evaluate the presence of lead calcifications. All patients were under general anesthesia in a hybrid surgical operating room. When IVL was used, it was performed using 7- and 8-mm balloons, and up to 300 pulses were delivered “in close proximity” to the leads being extracted. When the leads were freely mobile, the authors added, the case was excluded from this analysis.
The final cohort included 51 patients treated with conventional extraction and 14 patients treated using IVL lead extraction. The mean age for the conventional group was 67 years old, and 26% of patients were women. The mean age for the IVL group was 70 years old, and 21% of patients were women.
Overall, the use of IVL before TLE was associated with reducing the amount of time spent actively extracting leads by approximately 25 minutes. This is largely because pretreatment with IVL appears to minimize the need for power tools once the operator has successfully reached the lead.
The use of IVL does add approximately 15 minutes to the start of the case, however.
Reviewing the data, Latanich and Anderson concluded that additional research is still needed to learn more about IVL’s impact on both the safety and outcomes of TLE.
“This technique remains in its early stages of development overall and significant questions remain as to the overall safety with its use in the setting of retained leads, stenotic veins and within the heart,” the authors wrote. “Further studies are currently in the planning phases to assess these questions more systematically.”
Read the full study here.

Michael has more than 19 years of experience as a professional writer and editor. He has written at length about cardiology, radiology, artificial intelligence and other key healthcare topics.