
Cardiologists perform first TAVR of its kind by anchoring valve to crushed stent
Interventional cardiologists have performed the first transcatheter aortic valve replacement (TAVR) procedure of its kind on a patient with a failing noncalcified aortic valve. The group shared its experience in JACC: Case Reports.[1]
The patient, a 75-year-old woman, presented with shortness of breath and was confirmed to have severe aortic regurgitation (AR). She had a history of emergency cardiac surgery to treat an acute type A aortic dissection.
Cardiac CT images identified a dissection flap in the patient’s ascending aorta proximal to the surgical graft and signs of chronic aortic dissection from the aortic arch to the left iliac artery. After multidisciplinary heart team meetings, it was decided that surgical treatment would be associated with extreme risks. TAVR was associated with its own challenges, including “poor vascular access” and a high risk of coronary obstruction due to a residual ascending aortic flap.
The heart team finally concluded that TAVR with a balloon-expandable Sapien 3 valve from Edwards Lifesciences was their best option. Instead of a traditional TAVR, however, they made history by performing the very first anchoring via trans-leaflet apposition stent (ATLAS) procedure.
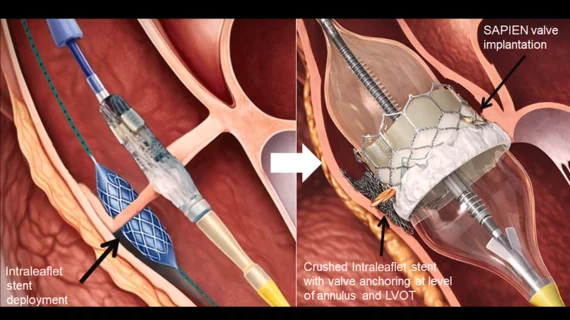
The ATLAS procedure was performed under general anesthesia, and sheaths were placed in the right axillary artery and right femoral artery. A Palmaz stent from Cordis was positioned inside the patient’s noncoronary cusp, and then the TAVR valve was placed inside the valve orifice and expanded, crushing the stent against the left ventricular outflow tract wall within the cusp. The TAVR valve frame was then anchored to the crushed stent.
Overall, the procedure was viewed as a success. The patient remained hemodynamically stable, and the axillary access site was closed with no issues. Valve stability and “device-stent interaction” were confirmed on both fluoroscopy and CT imaging.

Confirming valve-stent interaction. On (A) fluoroscopy and (B) computed tomography, the stent is shown to be flared above the aortic cusp (arrow), crushed in the left ventricular outflow tract, and mildly flared below the implanted Sapien 3 valve (dotted arrow). Images courtesy of JACC: Case Reports, Dvir et al.
“This first-in-human case highlights a novel anchoring strategy for TAVR in pure native AR, a clinical setting in which secure valve fixation remains a fundamental limitation,” wrote first author Danny Dvir, MD, an interventional cardiologist with Shaare Zedek Medical Center in Israel, and colleagues. “A critical component of the ATLAS technique is selection of the optimal leaflet and cusp for anchoring. This decision must balance mechanical stability with preservation of coronary flow and avoidance of interference with valve function. In our experience, the noncoronary cusp represents an attractive target for anchoring, given the absence of a coronary ostium, favorable fluoroscopic visualization, and its anterior orientation relative to the interatrial septum. These features may reduce the risk of coronary compromise and adjacent structural injury after stent deployment and subsequent crushing during valve expansion.”
Choosing the right stent is just as important, the group added. There can be no risk of the leaflet tearing, but the stent also needs to be strong and dense enough that can provide stable anchoring for the heart valve.
“It should be noted that although transcatheter vascular plugs may appear well suited for sealing gaps between adjacent structures, they do not provide comparable anchoring properties when crushed against another metallic frame,” the authors wrote. “Consequently, they are not considered suitable for the anchoring requirements of the ATLAS procedure.”
Cardiologists highlight the growing need for improved technologies
The group emphasized that TAVR valves specifically designed for noncalcified AR are still needed. “Innovative hybrid approaches” like ATLAS can make a difference, but they are also incredibly complex and do not represent a long-term solution for treating this vulnerable patient population.
“Dedicated AR platforms capable of reproducible leaflet engagement, accommodating large annular dimensions, and ensuring stable anchoring without reliance on calcification remain essential to safely expand the role of TAVR in the AR population,” they wrote. “Until such technologies are broadly available, techniques such as ATLAS may serve as valuable bridging solutions in carefully selected, high-risk patients.”
Click here to read the full analysis in JACC: Case Reports, an American College of Cardiology journal.

Michael has more than 19 years of experience as a professional writer and editor. He has written at length about cardiology, radiology, artificial intelligence and other key healthcare topics.