
Cardiologists propose new 'coronary risk zone' approach for redo TAVR planning
![A majority of medical devices involved in Class I recalls were never required by the U.S. Food and Drug Administration (FDA) to undergo premarket or postmarket clinical testing, according to new research published in Annals of Internal Medicine.[1]](/sites/default/files/styles/top_stories/public/2024-09/istock-1209664264.jpg.webp?itok=gQInU1vO)
Redo transcatheter aortic valve replacement (TAVR) volumes are on the rise, a trend that shows no signs of slowing down as TAVR continues to grow and become more common. Redo TAVR can be challenging, however, requiring a significant amount of preprocedural CT planning.
Hoping to simplify that complicated planning stage prior to redo TAVR, a team of valve implant specialists have collaborated on a brand new strategy designed to work with all transcatheter heart valves. The group shared this new technique in JACC: Cardiovascular Interventions, an American College of Cardiology journal.[1]
“This platform-agnostic approach simplifies redo TAVR planning into a single reproducible and easy-to-apply coronary clearance metric, which offers a rapid assessment to facilitate effective redo TAVR planning,” wrote first author Ole De Backer, MD, an interventional cardiologist with Copenhagen University Hospital in Denmark, and colleagues.
The proposed approach focuses on the “coronary risk zone” or CZR. The CZR sits between the neoskirt plane (NSP), defined as the top of the deflected leaflets, and the coronary risk plane (CRP), defined as the lowest point of each coronary ostium.
“Each coronary has its own CRZ, and this is the region in which we evaluate whether there is adequate space for coronary filling and catheter passage after redo TAVR,” the authors explained.
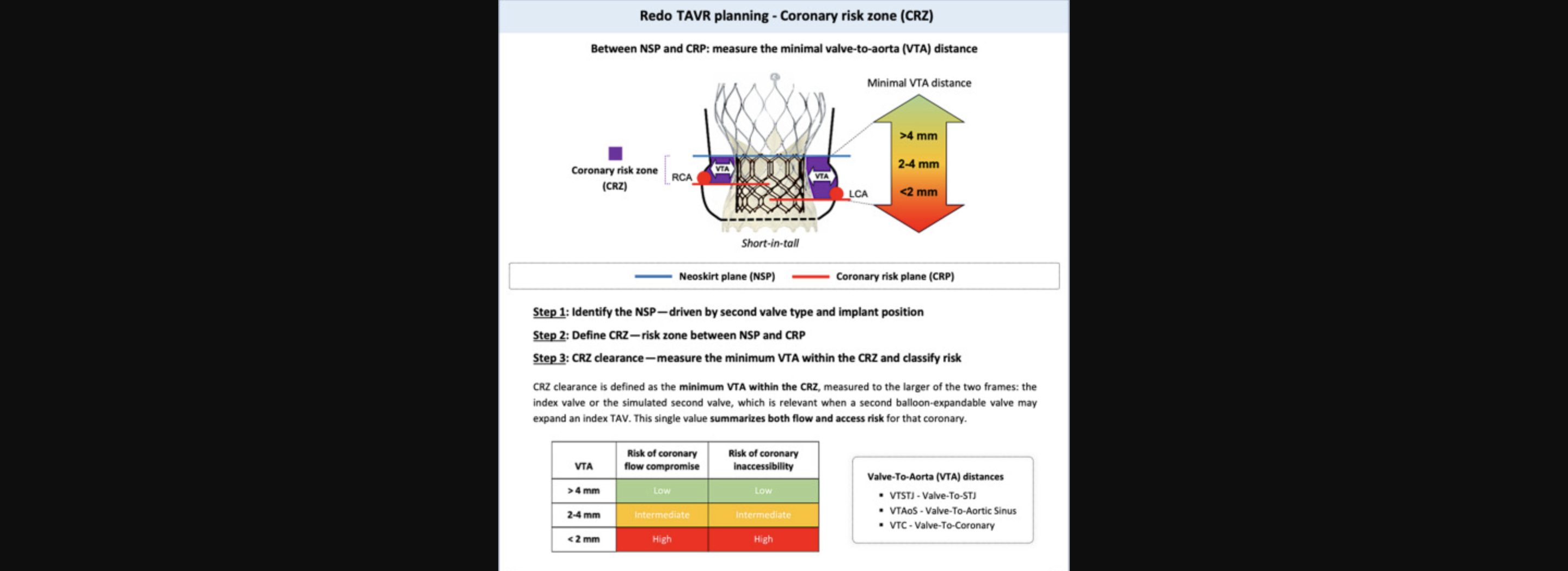
The three-step CRZ workflow includes: 1) identifying the NSP on the basis of the planned second transcatheter aortic valve (TAV-2) type and implantation position; 2) defining the CRZ from the relationship of the NSP to the CRP for each coronary; 3) measuring CRZ clearance for each coronary as the narrowest VTA distance to the larger of the index or simulated TAV-2 frame and classifying risk as low (>4 mm; proceed with redo TAV replacement [TAVR]), intermediate (2-4 mm; anticipate challenging access and consider mitigation), or high (<2 mm; consider platform or position change, coronary protection, and/or leaflet modification or surgery). Image and captions courtesy of JACC: Cardiovascular Interventions and De Backer et al.
The coronary risk zone workflow
The group identified three critical steps to the CRZ workflow:
- Identify the NSP
- Define the CRZ
- Evaluate CRZ clearance
Certain measurements and techniques will be specifically based on whether the second TAVR valve (TAV-2) has a short or tall frame. In addition, the authors emphasized that this proposed approach “does not replace detailed CT planning.” Instead, they explained, this simplifies the process by using standardized terminology and establishing specific thresholds that can guide the decision-making process.
“In practice, the CRZ gives operators a quick, practical language to communicate how small adjustments, such as lowering TAV-2 outflow in short-in-tall combinations or choosing a different TAV-2 platform or size to alter CRZ clearance, can change a redo TAVR procedure from unfeasible to high risk and even to low risk,” the authors wrote.
De Backer et al. also noted that intraprocedural aortic angiography is still “strongly recommended.”
The team did point to certain limitations, such as the fact that it does not account for the outward displacement of the patient’s native aortic valve leaflets. However, they believe this approach can make an immediate impact on patient care.
“The CRZ distills redo TAVR planning to a single, measurable clearance, helping standardize decision making across platforms, this while being adaptable to different device combinations and implantation strategies,” the authors concluded.
Click here for the full explanation of this new approach.

Michael has more than 19 years of experience as a professional writer and editor. He has written at length about cardiology, radiology, artificial intelligence and other key healthcare topics.