
New stroke prevention device for TAVR holds its own in head-to-head battle with Sentinel
A new-look embolic protection device for reducing the risk of stroke after transcatheter aortic valve replacement (TAVR) is associated with clinical outcomes comparable to Boston Scientific’s Sentinel Cerebral Protection System, according to new data presented at ACC.26 in New Orleans.
The device in question is the Emboliner Embolic Protection System from California-based Emboline. Features include a double-wall, cylindrical mesh filter made of Nitinol and a self-sealing port that allows devices such as TAVR delivery systems to pass through when necessary.
The ProtectH2H clinical trial was a head-to-head comparison of the Emboliner and Sentinel devices. It is believed to be the first head-to-head analysis of any two embolic protection devices for TAVR. More than 500 TAVR patients with a mean age of 79 years old were enrolled out of the United States, Germany and Brazil. Patients were excluded if they had experienced a stroke in the previous six months.
Adam Greenbaum, MD, an associate professor of medicine and co-director of the Structural Heart and Valve Center at Emory School of Medicine in Atlanta, presented his team’s data from the ACC.26 stage.
Overall, the head-to-head study showed that the Emboliner was noninferior to the Sentinel in terms of the composite primary endpoint of all-cause death, stroke or kidney failure within 30 days of TAVR. However, the Emboliner captured significantly more debris—three times as much, in fact—and was linked to an improved technical success rate.
This study was not specifically powered to examine the impact of capturing so much more debris, but this represents an area future studies could examine more closely. Greenbaum also noted that future research is already planned to see how this device may improve outcomes after other structural heart procedures.
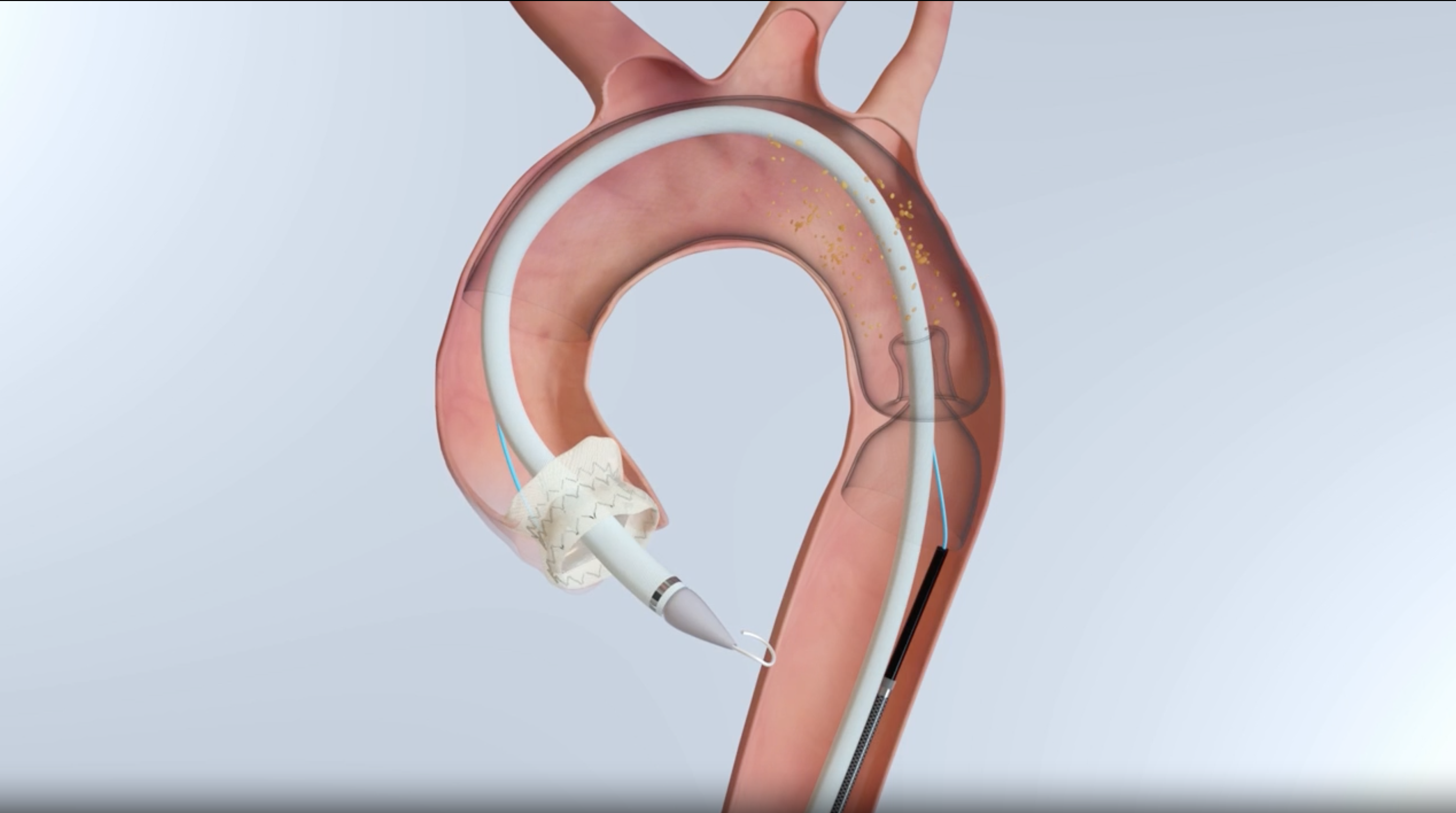
The Emboliner Embolic Protection System. Image courtesy of Emboline.
Are cardiologists getting closer to the ‘holy grail’?
Michael Young, MD, an interventional cardiologist with Dartmouth Hitchcock Medical Center, was on a panelist at ACC.26 when these findings were presented. He congratulated the research team and described eliminating the risk of stroke after TAVR as the “holy grail” in interventional cardiology.
“For those of us who perform TAVR and surgical aortic valve replacement (SAVR), I would argue that the patients who linger with us are the ones who have a major stroke after procedures that we do,” he said. “On a positive note, we have been better at periprocedural stroke rates over time … pretty good but not perfect. The idea is to predict and eliminate stroke completely, and that's what these trials and devices are hopefully meant to do.”
Young was also quick to point out the recent history of clinical trials focused on embolic protection during TAVR. Two studies, BHF PROTECT-TAVI and PROTECTED TAVR, failed to link cerebral protection with consistent across-the-board benefits in terms of risk reduction, though there were signs—in PROTECTED TAVR especially—that embolic protection may limit the risk of patients experiencing a major/disabling stroke. To this day, the use of the Sentinel device during TAVR procedures remains a bit of a controversy; some cardiologists want to use it during every procedure, but others think it may not be worth the extra time and added healthcare costs.
Greenbaum said the devices are clearly effective at collecting TAVR-generated debris when they are implanted correct and provide full coverage.” He also highlighted the fact that certain subsets of high-risk TAVR patients—those who undergo valve-in-valve procedures, for example—could potentially see significant benefits from the use of an embolic protection device.
“To me, any embolic debris during any procedure we do is neutral at best, but potentially harmful,” Greenbaum said. “If we had a device that was easy to place and highly technically successful, we should be able to show benefit.”
Emboline sees late-breaking data as an ‘important milestone’
“These results mark an important milestone for Emboline and support our belief that embolic protection in TAVR must address the full scope of embolic risk,” Scott Russell, president and CEO of Emboline, said in a company statement. “We designed the Emboliner to capture and remove debris while integrating seamlessly into procedural workflow, and we believe this combination differentiates the technology in structural heart. We look forward to submitting the study data for consideration of regulatory approval.”
“The liberation of embolic debris is ubiquitous in TAVR procedures, and these results support the safety and efficacy of a more comprehensive protection solution with the Emboliner,” added Tamim Nazif, MD, director of clinical research in cardiology at Columbia University Irving Medical Center and co-principal investigator of PROTECTH2H. “Importantly, the study also demonstrated the ease of use and high procedural success rates that are important in facilitating physician adoption of new devices.”
The Emboliner Embolic Protection System is not approved by the U.S. Food and Drug Administration at this time. However, Emboline is now working toward securing such an approval and commercializing the technology.

Michael has more than 19 years of experience as a professional writer and editor. He has written at length about cardiology, radiology, artificial intelligence and other key healthcare topics.