
TRILUMINATE update: TEER with Abbott’s TriClip device still safe, effective after 3 years

Abbott’s TriClip transcatheter edge-to-edge repair (TEER) system is still associated with positive patient outcomes three years after implantation, according to new follow-up data published in JACC: Cardiovascular Interventions.[1]
Background on TRILUMINATE
The TriClip device was designed to treat tricuspid regurgitation (TR) by clipping together flaps of tissue in the same way that Abbott’s MitraClip system targets mitral regurgitation. When it received U.S. Food and Drug Administration (FDA) approval in April, the agency’s decision was largely based on data from the TRILUMINATE clinical trial.
Overall, TRILUMINATE’s primary endpoint—a hierarchical composite that included all-cause mortality, tricuspid valve surgery, heart failure hospitalization and quality of life (QOL) improvements after one year—favored treatment with the TEER device. In addition, 98% of patients were free from major adverse events after 30 days, leading researchers to conclude that treatment with TriClip was safe.
Researchers share a 3-year update
This latest analysis represents the final follow-up of TRILUMINATE data, tracking data in 98 patients a full three years after treatment. All patients originally presented with moderate or greater symptomatic TR.
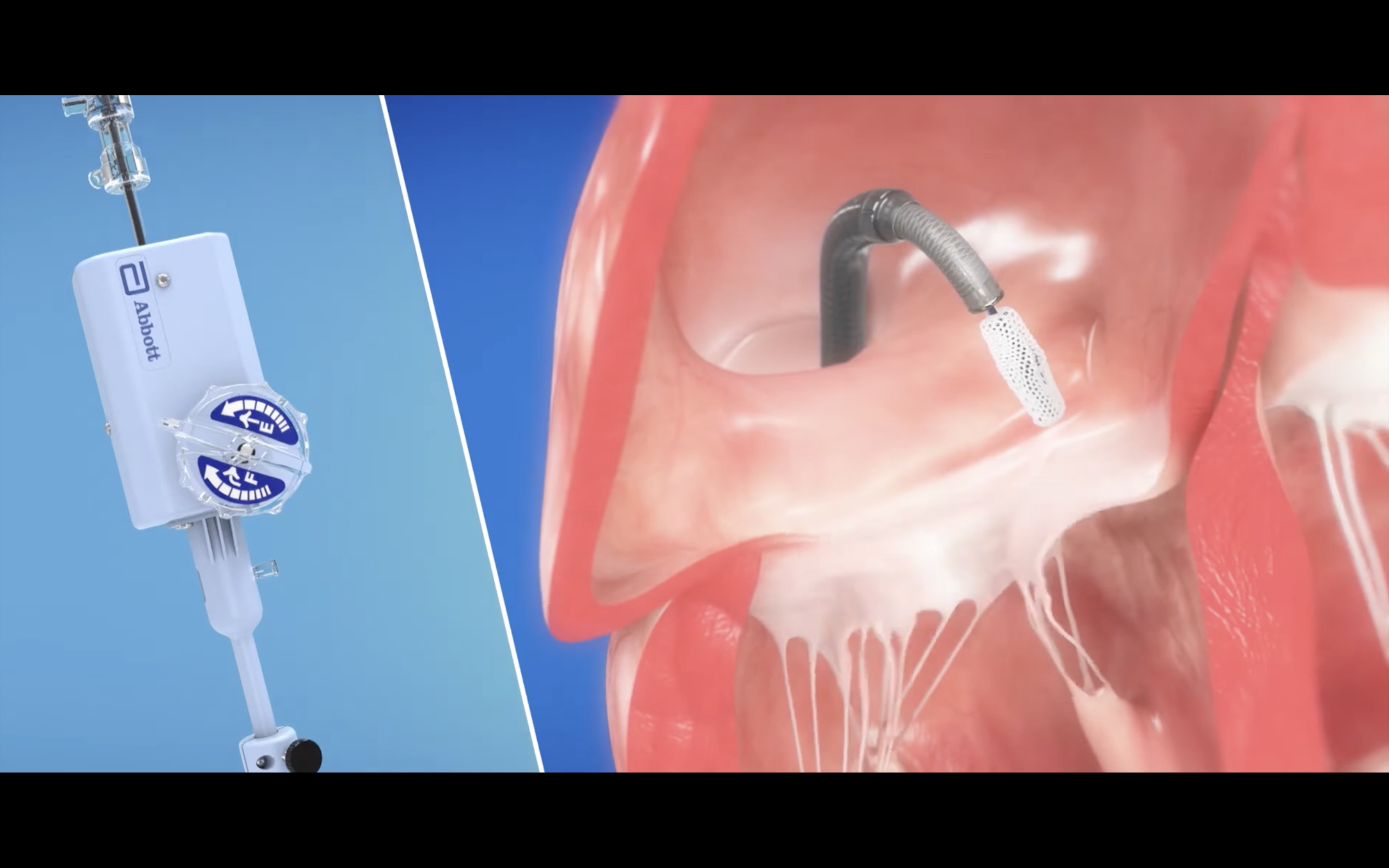
Abbott's TriClip device for TEER in patients with tricuspid regurgitation.
Overall, the group observed, TEER with TriClip reduced TR to moderate or less in 79% of patients. In addition, TR reduction seen after that first year was still seen after three years. Tracking heart failure symptoms and QOL questionnaires confirmed the team’s assessment that TEER was still a safe, effective treatment option. For example, the proportion of patients with New York Heart Association class III or class IV dropped from 76% at baseline to 19% after three years. Also, the major adverse event rate remained minimal, even after the full three years.
“The three-year outcomes demonstrate that subjects with symptomatic moderate or greater TR treated with TriClip show sustained benefits, including TR reduction and QOL improvements at three years,” wrote first author Georg Nickenig, MD, a cardiologist with University Hospital Bonn in Germany and co-author of the original TRILUMINATE study results, and colleagues.
Nickenig et al. also emphasized that “it remains unclear” if the TR reduction seen with TriClip significantly impacts a patient’s risk of mortality or hospitalization for heart failure symptoms; that is because the primary benefit identified in this analysis was related to QOL.
“However, our encouraging three-years results justify and warrant these further controlled studies on TEER in patients with severe, symptomatic TR, particularly in light of the favorable safety profile and the lack of other treatment options,” the group wrote.
Click here to read the full analysis in JACC: Cardiovascular Interventions, an American College of Cardiology journal. Co-authors included Gilbert H. Tang, MD; Rebecca T. Hahn, MD; Paul Sorajja, MD; and many others.

Michael has more than 19 years of experience as a professional writer and editor. He has written at length about cardiology, radiology, artificial intelligence and other key healthcare topics.