
Wearables & Workflow: How One Practice Is Hurdling Time, Liability & Billing

For Sanjaya Gupta, MD, MBA, the journey toward integration of consumer-level wearables into his cardiology practice began less than three years ago when an AFib patient came to him with a familiar story. The 70-year-old had recently undergone catheter ablation and was now mostly asymptomatic. Still, he was frustrated by not knowing if his heart was in or out of rhythm.
“He wanted more insight and control over his disease,” recalls Gupta, an electrophysiologist at Saint Luke’s Mid America Heart Institute and assistant professor of medicine at the University of Missouri-Kansas City. “We talked about the different types of monitors, including the relatively new AliveCor Kardia, which he could buy and attach to his phone. He lit up, and his wife was thrilled.”
What would have thrilled them even more was a way to show the patient’s recordings to their doctor. At that time, though, the technology was still “quite primitive,” with no easy way for a physician to access patients’ recordings or integrate findings into the EHR, Gupta says. As a short-term fix, the patient gave Gupta access to the online portal intended for customer use.
“That’s when I began to realize, if we could leverage this, it could be a really powerful tool,” says Gupta. Today, approximately 200 patients are regularly transmitting data from wearables to Saint Luke’s and another 100 are using the device on their own. “It’s growing,” Gupta says. “Two years ago, we had only three patients sending recordings.”
And, importantly, none of Gupta’s colleagues are complaining. “Physicians tend to resist wearables because they take time and expose them to some liability while giving them no compensation,” he says. “We addressed the time and liability hurdles, and we’re now the first clinic in the U.S. to automate the compensation process for reading consumerlevel wearables.”
Gupta told CVB why he believes in wearables and how he made the workflow work for himself and his team.
Let’s start with your first patient. Was he able to avoid any tests or procedures because he was taking readings that you could access?
Yes, we were able to drastically reduce the need for repeated cardiac monitors to give us a sense of how much AFib he was having.
There is currently no consumer-level device that provides continuous 24/7 monitoring of heart rhythms, but these devices give a more longitudinal perspective than prescribed devices, where the maximum is 30 days. You wouldn’t want to have a device attached to your skin for more than a month anyway. A patient can put the consumer devices in a pocket and use it whenever they want, across months or years. It’s helpful in a number of ways.
First, it’s a tremendous tool for patient engagement, particularly for patients whose AFib is largely asymptomatic. A wearable offers a window into what’s going on with them. They’re able to get tuned into their own health.
The wearable also gave my patient and his wife peace of mind, especially as he started to improve. In the first few weeks to months after an ablation, patients will go in out and out of rhythm. Managing that period can be difficult, but a wearable can make it easier on both patient and doctor. Without the wearable, a patient thinks he’s gone out of rhythm and calls the office. We need him to come in for an EKG. He needs to drive in, and we need to squeeze him into the schedule. Then the results must be interpreted, and the patient might have to drive back in for a cardioversion. In the meantime, his condition might have resolved. It becomes frustrating for everyone.
With wearable data, we can immediately correlate symptoms with the heart rhythm. It’s more efficient for everyone. Based on readily available information, I can decide whether to reassure my patient or have him come in for meaningful care.

How does hospital administration feel about you doing fewer EKGs?
No problem. The reimbursement for an EKG is very small. The loss of EKGs here and there is insignificant compared to the ability to provide better care, achieve huge patient satisfaction and improve overall efficiency in the system.
How do you decide which devices to trust and use?
It’s significant that, often, my patients are bringing new devices to me. They come in and show me what they’ve found. There are several devices that are just assessing regular vs. irregular heartbeat. That’s not diagnostic of AFib. That’s my first cut—does the device show an EKG-style report that I can interpret? If I can’t see what the device is thinking, then I don’t trust its diagnoses.
The second cut is whether the device is backed by data and FDA-approved. I can’t know the validity of a device that hasn’t been studied. That’s where the danger comes in. I like devices that show an EKG and have been FDA approved. So, for right now, that really narrows it. AliveCor and the Apple Watch are the two I use most frequently.
How are you obtaining informed consent?
Our lawyers approved a one-page document that patients sign if they are going to transmit recordings to us. It spells out who does what. They will send recordings. We will download them once per week and then get back to them within one week. If they are having symptoms, they need to call us. We will keep their information private and on a secure server.
Do you find that patients are overdoing it with the recordings? Or just quitting?
We do see new-toy phenomenon, where they do 100 recordings the first day. Some are just trying to learn it. That tends to taper off. Other patients will come in for an appointment and there’s only one recording per month in the portal. We explain that, to be useful, we need enough recordings to see trends. However, in the maintenance phase three months or more after an ablation, it can be fine if they just use it when they experience symptoms.
Have you noticed improved medication adherence in patients using wearable devices?
 We’re researching that very question—if wearables increase patient engagement, could they also change patient behavior? People who use a blood pressure cuff tend to do better taking their medications. Diabetics with their own glucose monitors do a better job watching their diet. AFib is less of a lifestyle disease than hypertension and diabetes, but taking medications is important. We’re conducting the Better Outcomes of Anticoagulation Treatment Through Observation of Atrial Rhythm (BOAT-OAR) to see if AFib patients who have a smartphone are more likely to take their blood-thinners if they are using an AliveCor monitor. We hope to present results in 2020.
We’re researching that very question—if wearables increase patient engagement, could they also change patient behavior? People who use a blood pressure cuff tend to do better taking their medications. Diabetics with their own glucose monitors do a better job watching their diet. AFib is less of a lifestyle disease than hypertension and diabetes, but taking medications is important. We’re conducting the Better Outcomes of Anticoagulation Treatment Through Observation of Atrial Rhythm (BOAT-OAR) to see if AFib patients who have a smartphone are more likely to take their blood-thinners if they are using an AliveCor monitor. We hope to present results in 2020.
You’ve said that getting the workflow right is the secret to success. Describe your workflow.
This is the most common question my colleagues ask. Naturally, physicians are apprehensive about adding more burdens on their clinics and staff. We had two priorities when we decided to get into consumer-level wearables. First, it has to be very easy for our patients. Second, the workflow must be in line with what our physicians and staff already know—in other words, what we’re already doing with event monitors.
Here’s how it works with AliveCor wearables: Patients get the device, sign our informed consent form and enroll with the service that gives us access to their portal. It costs $5 per month. From then on, they use the device like they would normally. That means they use the device to get recordings—no extra steps or need for them to transmit their recordings to us.
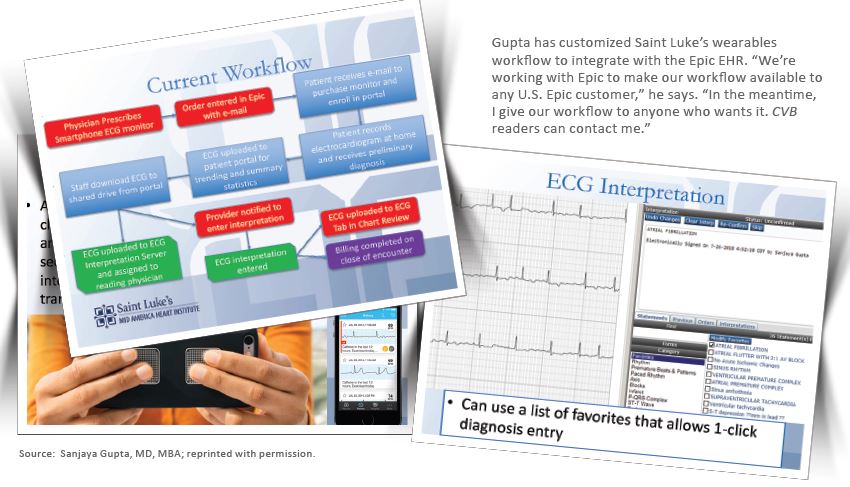
On the back end, the recordings go to the portal. The workflow starts with members of our office staff who have been trained to read EKGs and check event monitors. Once each week, they log on to the portal and downloads the recordings into the same software we use to read EKGs. They review the recordings, enter a preliminary diagnosis for each and assign each patients’ recordings to the prescribing doctor.
The physician gets a notice through the EHR to review recordings. We can launch the reading software and open the wearable recordings from within the EHR—just like for EKGs. We see a split panel with the recording from the patient on the left and a diagnosis checklist on the right. With one click, I can assign a diagnosis and move on. It’s fast, in line
with what I do and part of the same workflow as reading my EKGs.
But here’s the key to reducing the volume: We set a filter on the AliveCor portal to download no more than three recordings per day per patient and no more than two of the same rhythms per patient. You can customize the filter. You could start out seeing every recording and then restrict it to, for example, just abnormal recordings or just AFib with a heart rate of 120 or more beats per minute. Having these limits in place has made it a good experience.
Does it work the same with the Apple Watch?
No, Apple doesn’t have an application programming interface, so there’s no portal and, therefore, the workflow isn’t there yet. Patients bring in their Apple Watch and we review it. We’re interested in working with Apple to develop a portal because it will help us take better care of patients. That’s the major reason we recommend the AliveCor device more than the Apple Watch. Plus, the Apple Watch costs more. Through Epic, we’re working with Apple on a schematic that would let us export EKGs through the Apple Health Kit (an iPhone app) to the EHR, but this is still under development.
How have you automated the billing?
Remember, we’re reading the recordings from within the EHR. So, once the physician reads a recording and clicks the diagnosis, the information is integrated, just as it is with an event monitor. That step also triggers automatic billing. The order type is linked to the specific charge.
There are two ways to bill. First is on a per-EKG basis. Our professional fee for interpretation is $20 per recording. If you read 20 recordings from a patient, you bill for 20 EKGs. The average reimbursement ranges from $5 to $12, depending on the payer. We've found about 80 percent of our AliveCor Kardia interpretations are being paid by insurers.
The other way is to use the billing code for comprehensive remote patient management. We’ve just begun using this code. It involves a physician or staff spending at least 30 minutes reviewing data transmitted by a patient and then talking to the patient about the results. This is billed monthly and is valued at a higher rate than reading EKGs.
What’s your advice to colleagues who aren’t sure about joining the wearables movement?
First, don’t be afraid of data overload. This can be done seamlessly without overloading your staff while making it easier to take care of your patients and getting your patients more engaged.
Second is that wearables are new, but our fears aren’t. We’re afraid of people mismanaging or misinterpreting the data and drawing the wrong conclusions. We’re worried about false-positive findings leading to panic. Those aren’t new fears. We worried about it with home-based blood pressure cuffs and self-monitors for glucose. Now, we use them all the time. With all of these things, including the new wearables, patients must be involved in the discussion. They trust their doctors and will listen to us. Tell your patients, “This is how and when I want you to use this device. If you see this result, call me.” The vast majority of people will be grateful and use the devices appropriately.

Kathy joined TriMed in 2015 as the editor of Cardiovascular Business magazine. She has nearly two decades of experience in publishing and public relations, concentrating in cardiovascular care. Before TriMed, Kathy was a senior director at the Society for Cardiovascular Angiography and Interventions (SCAI). She holds a BA in journalism. She lives in Pennsylvania with her husband and two children.