
Look Before You Leap & Other Advice for Cardiologists Considering Telemedicine

Telemedicine use continues to expand, offering opportunities for cardiologists, practices and health systems. What’s less clear is how much it’s expanding and, therefore, just how big the opportunities really are.
Part of the challenge is language. Telehealth and telemedicine are often, but not always, used interchangeably. The American Telemedicine Association (ATA) explains, “While some have parsed out unique definitions for each word, ATA treats ' telemedicine and 'telehealth’ as synonyms ... In both cases, we are referring to the use of remote health care technology to deliver clinical services.”
Because some have ascribed differences to the nomenclature, surveys conducted at similar time intervals, even in like populations, have sometimes yielded contradictory findings. “It’s very confusing,” says Heba Wassif, MD, MPH, Cleveland Clinic cardiologist, long-time telemedicine practitioner and member of the American College of Cardiology (ACC) Health Care Innovation Council.
The ATA echoes her assessment on its website: “Estimates on the market size for telemedicine vary widely, depending on each analyst’s precise definition of telemedicine. While they can’t agree on a single number, one area where all research firms concur is that the telemedicine market is growing rapidly.”
Showcasing the variation in results are surveys conducted by two companies over the past five years:
› In 2019, telehealth company American Well found that 22 percent of physicians have used telehealth to see patients. That’s up from 5 percent in 2015.
› Data from Definitive Healthcare surveys showed hospitals and health systems increased telehealth adoption from 54 percent in 2014 to 85 percent in 2019. In contrast, use by physician practices dropped from 49 percent in 2017 (the first year Definitive Health included practices in its surveys) to 44 percent in 2018 and 2019.
Despite Definitive Healthcare’s second finding, experts feel sure that telemedicine use will continue to expand, and they’re urging physicians to get ready.
Conflicting signals
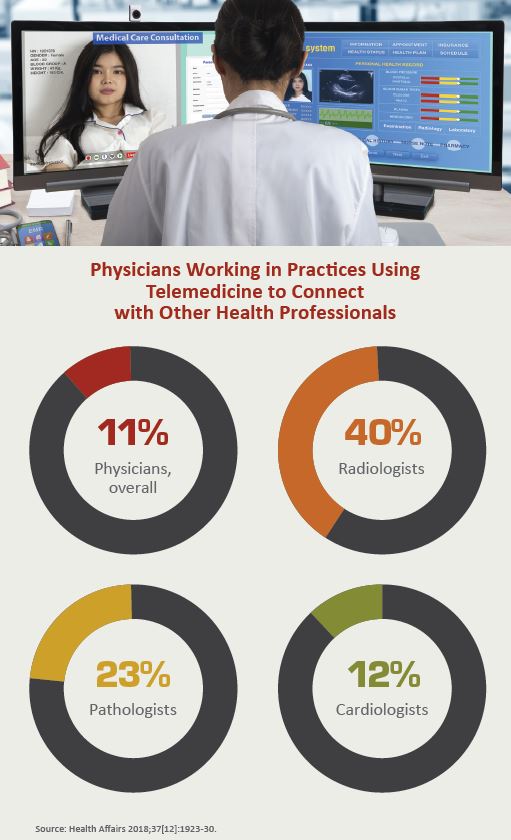
A 2018 Health Affairs study revealed wide variation in telemedicine use across specialties, with cardiology lagging behind some other fields on specific data points. In 2016, for example, 40 percent of radiologists and 28 percent of psychiatrists—vs. only 24 percent of cardiologists—were working in practices that used telemedicine for patient interactions. Cardiologists were more likely than most physicians to be working in practices leveraging telemedicine for staff interactions, but they came in behind radiologists and pathologists on this metric (37[12]:1923-30).
By some standards, however, cardiology is an early telemedicine adopter. Cardiac rehab and remote cardiac monitoring have “laid the important groundwork for advancing use of the technology,” says Elizabeth Siemsen, director at AMGA (formerly the American Medical Group Association).
The Health Affairs findings sync with this conclusion: Among the surveyed cardiologists, 18 percent were in practices using remote patient monitoring, and 19 percent were using telemedicine to manage patients with chronic disease. And now telemedicine procedures are gaining traction, as evidenced by the first truly remote PCIs performed on humans—with the patients as far as 20 miles away.
While the technology fueling telemedicine still has hurdles to overcome, it’s not the biggest barrier. As the Center for Connected Health Policy warns, no two states define, reimburse or regulate telehealth/telemedicine the same way.
Licensing frustrations
According to the Federation of State Medical Boards, 49 state boards, plus the boards in Washington, D.C., Puerto Rico and the Virgin Islands, require physicians engaging in telemedicine to be licensed in the state in which the patient is located.
This requirement can make some of the simplest encounters tricky, observes Eric C. Stecker, MD, MPH, an Oregon Health & Science University (OHSU) cardiologist whose practice is in Portland. “Many of my patients live just across the river in the state of Washington,” he notes.
A similar geography challenge emerges when patients travel. EHRs document where patients live but are unlikely to note if they winter in Florida.
Some states are trying to make it easier. Nine state boards now issue special licenses or certificates related to telehealth, which, under certain circumstances, allow out-of-state practitioners to provide telemedicine services in a state where they are not located or allow clinicians to provide services in the state (Perm J 2019;23:18-29). The Interstate Medical Licensure Compact offers an expedited pathway to licensure for qualified physicians to practice in most states; 27 states, Washington, D.C., and Guam have joined the Compact.
In addition, a rule that went into effect in 2018 allows Veterans Administration providers to treat veterans regardless of the veteran’s or the provider’s location.
While prospective telemedicine providers shouldn’t ignore licensing challenges, the key is for them to focus on compliance requirements just as they do for in-person visits, experts say. Here’s how:
Malpractice & liability: Different mode, same diligence
“I would say just a basic amount of due diligence can go most of the way to avoiding all the risks,” says Stecker, who sees patients remotely and works with the OHSU’s Knight Cardiovascular Institute to extend specialty consultative care. The issues are actually quite simple, Stecker adds, but they cannot be overlooked. because “the potential ramifications are huge.”
Compared to other modes of remote interaction, telemedicine more easily establishes a doctor-patient relationship, he warns. “And of course, once the doctor-patient relationship is established, there are obligations that go along with it.” If those obligations aren’t met, he emphasizes, “one is at risk for malpractice lawsuits.”
It comes down to this, say experts: Document appropriately and follow the same standards of care you would for in-person encounters.
The same recommendation applies on the regulatory side, says Adrienne Lloyd, MHA, MGMA consultant and CEO/founder of Optimize Healthcare. “Physicians need to do similar documentation and close the loop as they would for a normal in-person visit.” She hasn’t seen any additional scrutiny of telemedicine providers.
But there is scrutiny.
In April 2018, the U.S. Department of Health and Human Services Office of the Inspector General (OIG) issued a report with the revealing title, CMS Paid Practitioners for Telehealth Services That Did Not Meet Medicare Requirements. The OIG reviewed a sample of 100 claims and found 31 did not meet Medicare requirements. Two categories stood out:
› Receiving services at non-rural sites, and
› Services billed by ineligible institutional providers
As with any new endeavor, practices should take the time to research what’s involved before taking the plunge.
“When I first got into telemedicine, I had to spend a long time educating myself about its practice laws, reimbursement models, etc.,” says Mohamed B. Elshazly, MD, cardiologist and assistant professor of medicine at Weill Cornell Medicine-Qatar, who co-founded the telemedicine firm Ember Medical and is a member of the ACC’s Digital Health and Devices Work Group. “I wish learning about this could be incorporated into our medical education or graduate medical training. We need to learn more about its tremendous potential as well as the risks.”
Compensation, reimbursement & value
“The compensation picture for telemedicine is still foggy but is becoming clearer,” says Fred Horton, MHA, president of AMGA Consulting. He points to findings from the organization's 2019 Medical Group Compensation and Productivity Survey. Of those using telemedicine, 49 percent of respondents said they were reimbursed for e-visits in 2018, and 44 percent reported capturing wRVUs for telehealth visits.
Meanwhile, reimbursement is improving, especially since Medicare unveiled new codes for remote consults and virtual check-ins. But although most states now have coverage parity, they don’t have payment parity.
As CVB reported in January, virtual hospitals are gaining traction, but most aren’t turning much of a profit. They’re having more success in risk-based models, which pay for value over volume—and not based on the visit’s location.
In a fee-for-service world, it remains difficult to make a profit with telemedicine, but that has been changing, too. Telehealth adoption accelerates rapidly with the transition from volume to value, according to the 2018 report Accelerating Telehealth Adoption: Telemedicine's Role in the Volume to Value Journey by the nonprofit accreditation organization URAC.
Experts concur, with Elshazly estimating that cardiology could probably shift more than half of its follow-up appointments to telemedicine and remote monitoring. But doing so will depend on creating the business case and selling it.
The business case
For health systems in the midst of consolidation, telemedicine is a way to keep patients in the fold, says AMGA Consulting’s Siemsen. Telemedicine encourages patients to stay in the system, even after a clinic or service line closes. Ideally, this leads to optimal outcomes at the lowest costs.
Stecker agrees, noting that in regions suffering cardiology shortages, telemedicine “really allows a very different level of expertise to be brought to areas where normally it would not be available.”
Even if practices and health systems wanted to locate nearer to these communities, setting up satellite clinics can be prohibitively costly, he adds.
Costs, efficiencies and logistics aside, telemedicine’s primary appeal for physicians is its potential to increase access to medical care for patients, according to Stecker. “I think many, many cardiologists take great pride in their judgment in the procedures and the services that they can offer,” he says. “Telemedicine allows them to extend their reach efficiently.”
Work from anywhere?
Aside from licensing requirements, telemedicine doesn’t really hinge on where the physician is located. That makes it appealing to some cardiologists. “They could do this when they are traveling, or make their Fridays be a work-from-home—or work-from-wherever—day and batch a bunch of e-consults, if they have consistent internet,” Lloyd says.
Wassif also appreciates the flexibility telemedicine offers physicians but advises against being too casual about it. “You can’t do it from the kitchen,” she says.
While telemedicine is usually considered in the context of practices and health systems, it also can provide a moonlighting opportunity for physicians. They contract with a company such as Teladoc, Doctor on Demand, AmericanWell or MDLive. With these arrangements, Elshazly explains, physicians typically are paid a flat fee and the company then bills the payer. The result for physicians is an income boost and relief from much of the administrative burden.
In these models, physicians don’t have much, if any, input on which patients are seen via telemedicine visit. With their own patient panels, physicians should carefully consider whether individual patients are a good fit.
Choose patients wisely
Cardiologists should be “very discerning” about patient selection for telemedicine, Wassif emphasizes, and that means confirming that both the condition and the patient are suited to telemedicine. Discuss how telemedicine works with each patient and be sure it’s appropriate for him or her, she says. Decide, also, which visits lend themselves to telemedicine—for instance, she never uses telemedicine for an initial visit.
Some physicians worry that telemedicine means losing the human touch in patient interactions, Wassif says. “I don’t think that is true,” she adds. “That’s where patient selection and communication is important.”
In fact, telemedicine can open up new opportunities for patient and family engagement, according to Lloyd. For example, she notes, a telemedicine visit could be configured to include both an elderly patient in North Carolina and her daughter in California. Lloyd says such encounters are becoming more common.
Getting started
Telemedicine can be an attractive path for cardiologists, but practices shouldn’t jump in too quickly, sources told CVB. Think it through, and include the administrative team in the deliberations, counsels Lloyd. There are various ways to incorporate telemedicine, and it’s worth investing time to find the one that fits their situation. “Done right, it’s a lifestyle-enhancer,” Lloyd says. But merely bolted on to a currently busy practice, “it could be a logistical nightmare.”
Fortunately, there are examples of how to do it right, Stecker says. “Look at how others have done it in other places, and use that as a template you can adapt to what you want to do.”
Then take the plunge.
“I wish cardiologists would lead the way and take matters into their own hands in designing telemedicine best practices for our own specialty,” Elshazly says. “We must identify where we think telemedicine can be most beneficial to our patients, figure out how to apply it. We must to take the lead rather than being stuck in the status quo.”