
A leadless pacemaker the size of a grain of rice delivers cardiac resynchronization therapy
Results from a pivotal clinical trial presented as a late-breaker at Heart Rhythm 2023 indicate that a new leadless pacemaker technology can deliver cardiac resynchronization therapy (CRT) among patients who were not able to be treated with conventional CRT and epicardial leads.
For many patients with heart failure, their two ventricles end up beating at different times in a dyssynchronous rhythm. The current standard of care to achieve synchrony is CRT, which uses pacing to synchronize the contraction of the right and left ventricles. However, lead-based pacemakers have known limitations and up to 30% of patients fail to benefit from this therapy.[1] This trial was designed to address that population.
The SOLVE-CRT study was a prospective, international, multicenter pivotal trial that included a randomized arm and a subsequent single-arm. The randomized part of the study initially intended to enroll 350 patient participants for three indications. This included patients who were non-responders (NR), those previously untreated, including acute and chronic lead failures (PU), and patients undergoing high-risk upgrades (HRU) from existing implanted cardioverter defibrillators (ICD). All participants underwent device implantation and were then randomized in 1:1 ratio to treatment (system turned on) or control (system turned off) groups. A total of 108 participants were enrolled by March 2020 when enrollment was halted due the COVID-19 pandemic.
The single arm part of the study was approved by the U.S. Food and Drug Administration (FDA) during the COVID-19 pandemic and was designed to enroll up to an additional 192 participants within two indications of PU and HRU. An interim analysis was conducted after 75 participants were enrolled. Data from all 183 participants in both parts were included in the interim safety analysis.
The primary safety endpoint for the SOLVE-CRT study was freedom from Type I (device and procedure-related) complications through six months. Efficacy analysis included all participants in the single arm (75) and those randomized to treatment from the PU and HRU groups only (25), for a total of 100. The primary efficacy endpoint was the improvement in left ventricular systolic volume (LVESV). The study looked at the impact of the EBR system in preventing reverse remodeling, which was set at changing the end systolic volume below a threshold of 9.3%.
"We had a success rate of 16.4%, so we really beat that threshold," Singh explained in an interview with Cardiovascular Business.
The WiSE CRT was shown to be safe with an 80.9% freedom from Type I complications from the system and the procedure.
Since both primary endpoints were met at this interim analysis, study enrollment was concluded early.
"Because heart failure is a progressive disease, patients who fail conventional CRT experience worsening symptoms that can result in repeated hospitalizations and reduced life expectancy. The results of SOLVE-CRT offer a new hope for patients with hard-to-treat heart failure," said co-PI of the study Jagmeet Singh, MD, of Massachusetts General Hospital, Harvard Medical School, along with Mary Norine Walsh, MD, with Ascension St. Vincent Heart Center in Indianapolis, Indiana. "Endocardial leadless pacing will allow physicians to choose where to implant the device within the left ventricle and give them the ability to tailor the therapy directly to each individual patient’s needs."
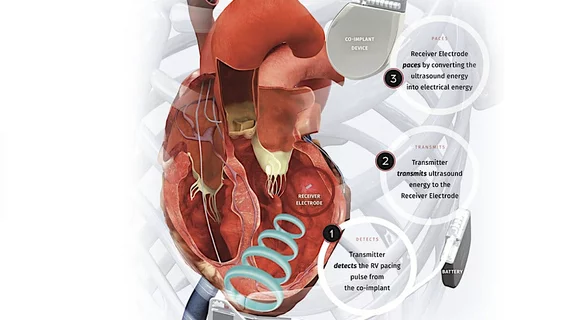
How the leadless CRT pacing technology works
The EBR Systems Inc. WiSE CRT system works in concert with existing implanted device that can pace the right ventricle. The WiSE system is a wireless receiver electrode that is about the size of a large grain of rice. It is implanted into the left ventricle's endocardium. Singh said this can be implanted transseptally or retrograde through the aorta. The receiver is then stimulated by an ultrasound transmitter implanted subcutaneously just beyond the midaxillary line, which is powered by an implanted battery pack. The electrode coverts the ultrasound energy into electrical energy to enable pacing.
"It is a really novel technology that now allows us to pace the left ventricle and resynchronize it in a leadless fashion," Singh explained. "I think the advantages are that it allows a more refined targeting or wherever you want want to place the electrode. Second, it is actually endocardial pacing, so it resynchronizes better. The third advantage is that you now have the potential for a completely leadless resynchronization therapy system."
The sponsor of this trial, EBR Systems Inc., is currently working to submit the data from this trial for an FDA premarket approval (PMA).

Dave Fornell has covered healthcare for more than 17 years, with a focus in cardiology and radiology. Fornell is a 5-time winner of a Jesse H. Neal Award, the most prestigious editorial honors in the field of specialized journalism. The wins included best technical content, best use of social media and best COVID-19 coverage. Fornell was also a three-time Neal finalist for best range of work by a single author. He produces more than 100 editorial videos each year, most of them interviews with key opinion leaders in medicine. He also writes technical articles, covers key trends, conducts video hospital site visits, and is very involved with social media. E-mail: dfornell@innovatehealthcare.com