
Radiation doses during heart scans vary dramatically from one country to the next

A new cross-sectional study of 742 centers in 101 countries involving the International Atomic Energy Agency (IAEA) offers the first world-wide glimpse into radiation dose variations used in coronary artery diagnostic imaging.
The analysis, published in JAMA, identified a wide variation in dose among these centers, with the highest doses in middle- and low-income countries.[1]
The IAEA Noninvasive Cardiology Protocols Study (INCAPS) 4 included 19,302 patients who underwent noninvasive coronary imaging. Participating sites reported their the cardiac imaging data for a one-week period between the weeks of Oct. 15 and Dec. 10, 2023. This included single-photon emission computed tomography (SPECT), positron emission tomography (PET), Coronary artery calcium scoring (CACS) or coronary CT angiography (CCTA). The goal was to assess radiation doses for noninvasive coronary artery disease (CAD) imaging around the world to help identify actionable areas for improvement.
The study found that significantly more centers are performing nuclear imaging studies than CCTA (81% vs. 56%). These exams achieved a median dose of less than or equal to 9 mSv.
Radiation doses for the same procedure varied widely between regions, researchers found. Western Europe had the lowest median doses of 4.8 mSv for nuclear cardiology and 4.6 mSv for CCTA. The highest median dose for nuclear cardiology was in Latin America (7.8 mSv) and Africa had the highest median dose for CCTA with a whopping 25.2 mSv, 500% higher than what is seen in Western Europe.
Overall, the median dose for CCTA in low- and lower-middle–income countries was more than 280% higher than what is found in high-income countries. Patient dose was 20% higher in low- and middle-income countries than in high-income countries for nuclear cardiology, and as much as 96% higher in low- and lower-middle–income countries than in high-income countries for CCTA. There was also notable variation within income levels and world regions.
"Given increasing rates of CAD worldwide, these findings of marked variation in radiation dose to patients from diagnostic testing identify a critical need for training, standardized protocols and updated equipment to reduce radiation world-wide," wrote lead author Andrew J. Einstein, MD, PhD, director of nuclear cardiology, cardiac CT and cardiac MRI and a professor of medicine in radiology at Columbia University Irving Medical Center/NewYork-Presbyterian Hospital, and colleagues.
Einstein spoke to Cardiovascular Business about the data, saying this research serves as a benchmark to measure future progress. He also pointed to the fact that radiation doses for cardiac testing exceeded 9 mSv for 21% of patients undergoing nuclear cardiology exams and 44% of patients undergoing CCTA. This needs to be lowered to improve patient safety and prevent radiation-attributable cancers, he explained.
"This was the broadest study with countries across the globe, including some never included before from places like Nicaragua and Fiji," Einstein said. "There was a lot of variability between regions."
What explains these large differences in radiation dose?
Einstein said there are reasons for significant variations at centers with very high radiation dose levels, and it does not necessarily mean they are not following best practices. For example, doses might be high because the technologies are old, not because of any lack of effort.
"That's not bad radiation; it is good radiation, because it is needed to get a diagnostic-quality image," he said.
While the median dose of CCTA was 5 mSv at 37% of centers performing CCTA, 24% of centers were still using CCTA doses of more than 15 mSv. African centers had a median 25.2 and overall higher dose rates of between 14.7-35.3 mSv.
"It's a combination of factors. Some have older technology and others focus on higher doses to boost image quality," Einstein explained.
The median African dose for CCTA is very high compared to what is seen in the U.S. today, but Einstein noted that 20 years ago when CCTA began to be used in the U.S., it was not uncommon to see doses around 25 mSv. This was in a time before iterative image reconstruction and using single source CT systems with retrospectively gated exams. But CT technology has evolved a lot in the intervening decades, with prospectively gates exams that modulate the energy levels when imaging is captured during optimal portions of the cardiac cycle based on ECG, more sensitive detectors, scanners with more than 64 slices and wider anatomical coverage per rotation, faster scan times, noise reduction technology, iterative reconstruction and AI-aided image reconstruction. This has enabled much lower dose scans
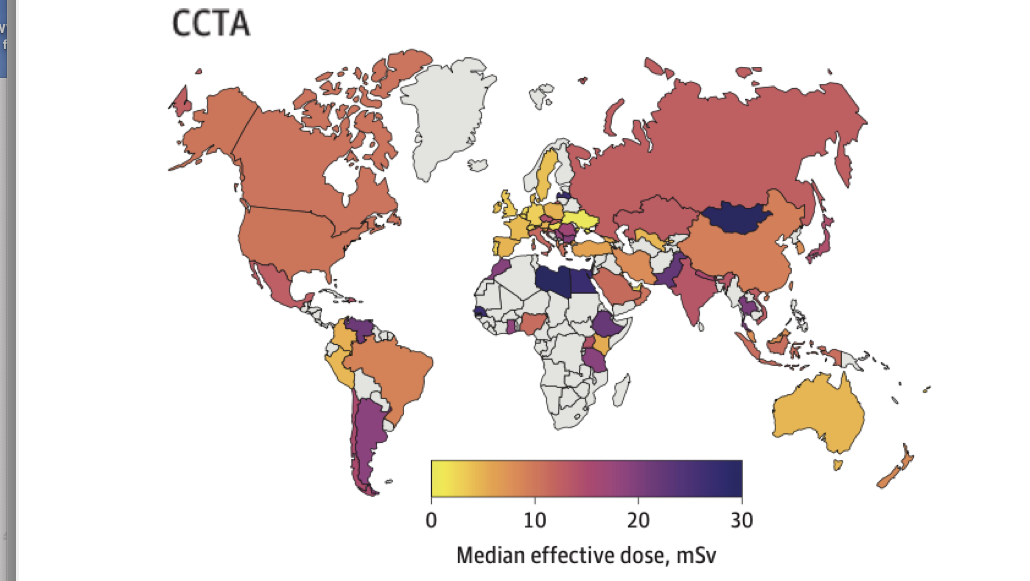
Image courtesy of JAMA.
Compared to studies of U.S. dose levels in the past, both CCTA and nuclear imaging saw significant drops in median dose in this study from what average levels were a decade ago. Einstein attributed this largely to the adoption of newer imaging technologies the use of optimal techniques. While acknowledging the positive decline in dose, Einstein did note this study was not meant to be a comparison of dose levels across time or between modalities.
"So the technology has definitely changed to enable lower radiation doses. With new technology, you can do better things for your patients" he said.
Beyond regional variations, the study also showed a fair amount of variability in doses used for the same types of patients between operators. He said that needs to be addressed with training and operators paying more careful attention to dose-lowering techniques.
"It is a shared responsibility of the physicians and the technologists conducting the exam to strike a balance for the best dose for each patient," Einstein said.
Study shows real-world cardiac imaging dose globally
Many previous studies on radiation dose focused on larger, luminary centers, which often cherry-picked data and presented what was not a true reflection of real-world dose levels at most smaller, non-academic hospitals. While major academic centers with large volumes of patients, the best imaging experts and newest technology can perform scans in the 1-5 mSv range, the routine scanning dose at most centers is higher. He said this is partly due to the use of older technologies and not always using the latest imaging techniques to closely modulate dose based of specific patient characteristics.
"If you just do a study on the experts you will not have a clear picture of CCTA use across the globe," he said. "This study certainly had a major focus on having the biggest reach possible globally."
How researchers estimated radiation dose
There are a variety of measures and calculations used to estimate radiation dose in medical imaging. The centers in this study collected included radiopharmaceutical administered doses for nuclear cardiology, and dose-length product (DLP) and volume CT dose indices for CCTA. The IAEA used this data to calculate the effective dose for each nuclear procedure using coefficients of millicurie (mCi) dosing of radiopharmaceuticals. It calculated each CT procedure by multiplying the DLP by an updated conversion factor for cardiac imaging (0.026 mSv × mGy−1cm−1), which Einstein said includes considerations for technologies used in current generation scanners and tissue-weighting factors.
Researchers found the following median radiation dose ranges based on modality and country income level.
Median dose ranges in high-income countries:
Nuclear cardiology: 3.9-8.2 mSv
CACS: 0.7-2 mSv
CCTA: 3.5-11 mSv
Median patient dose across income levels:
• Nuclear cardiology:
7.1 mSv in low/lower-middle–income,
6.4 mSv in upper-middle
6.1 mSv in high-income countries
• CACS:
1.7 mSv upper-middle–income countries
1.1 mSv high-income countries
• CCTA:
15.9 mSv low- and lower-middle income countries
10 mSv in upper-middle–income countries
5.6 mSv in high-income countries

Dave Fornell has covered healthcare for more than 17 years, with a focus in cardiology and radiology. Fornell is a 5-time winner of a Jesse H. Neal Award, the most prestigious editorial honors in the field of specialized journalism. The wins included best technical content, best use of social media and best COVID-19 coverage. Fornell was also a three-time Neal finalist for best range of work by a single author. He produces more than 100 editorial videos each year, most of them interviews with key opinion leaders in medicine. He also writes technical articles, covers key trends, conducts video hospital site visits, and is very involved with social media. E-mail: [email protected]