
A new alternative: Surgeons, cardiologists gather to learn about robotic aortic valve replacement

Specialists at West Virginia University (WVU) are once again hosting an international symposium focused on educating cardiac surgeons and cardiologists alike about robotic aortic valve replacement (RAVR).
The WVU Heart and Vascular Institute hosted its first RAVR symposium in 2024, and the two-day event was a big success. The 2025 edition of the WVU International RAVR Symposium is scheduled for Nov. 13-14. It will feature live cases, keynote speakers, group discussions and more.
The steady rise of RAVR
RAVR is a new minimally invasive treatment option for patients with symptomatic severe aortic stenosis. The procedure pairs the benefits of transcatheter aortic valve replacement (TAVR)—no sternotomy, for example—with the proven long-term outcomes of surgical aortic valve replacement (SAVR).
Vinay Badhwar, MD, executive chair of the WVU Heart and Vascular Institute and chair of the WVU School of Medicine’s department of cardiovascular and thoracic surgery, helped develop a RAVR technique that is now being used by heart teams all over the world. He also serves as the symposium’s program director. Badhwar told Cardiovascular Business that it is still the early days of RAVR—approximately 400 cases have been performed so far—but enthusiasm for the procedure is steadily rising.
One of the most important things with RAVR, Badhwar said, is that it stays safe and it stays reproducible.
“We have been honored to embrace and support the adoption of RAVR across multiple institutions and multiple countries," he said. "However, whether RAVR is performed in Morgantown, Miami or Milan, we have suggested that the technique should be similar. The premise of our early papers and the multi-institutional experience on RAVR was that we would always stay consistent with our techniques. This has enabled consistency and quality reporting as it has expanded across institutions.”
For Badhwar and his team at WVU, RAVR has become as routine as other cardiac procedures. Other care teams around the world are starting to gain more and more experience as well. One reason for that trend seems to be how quickly information is spreading about RAVR online. For example, Badhwar noted that surgeons used to call him up if they were interested in RAVR, because they wanted to fly to WVU and watch his team in person. Now, however, he said surgeons interested in RAVR are just as likely to look up online videos and start looking into performing cases of their own.
Badhwar did emphasize that a basic understanding of robotic surgery is necessary for anyone considering RAVR. Experience with the equipment is crucial, for instance, if you are going to carry out the precise movements required to robotically replace a patient’s heart valve. Other than that one caveat, however, he feels that this is a procedure anyone with the proper training can safely perform.
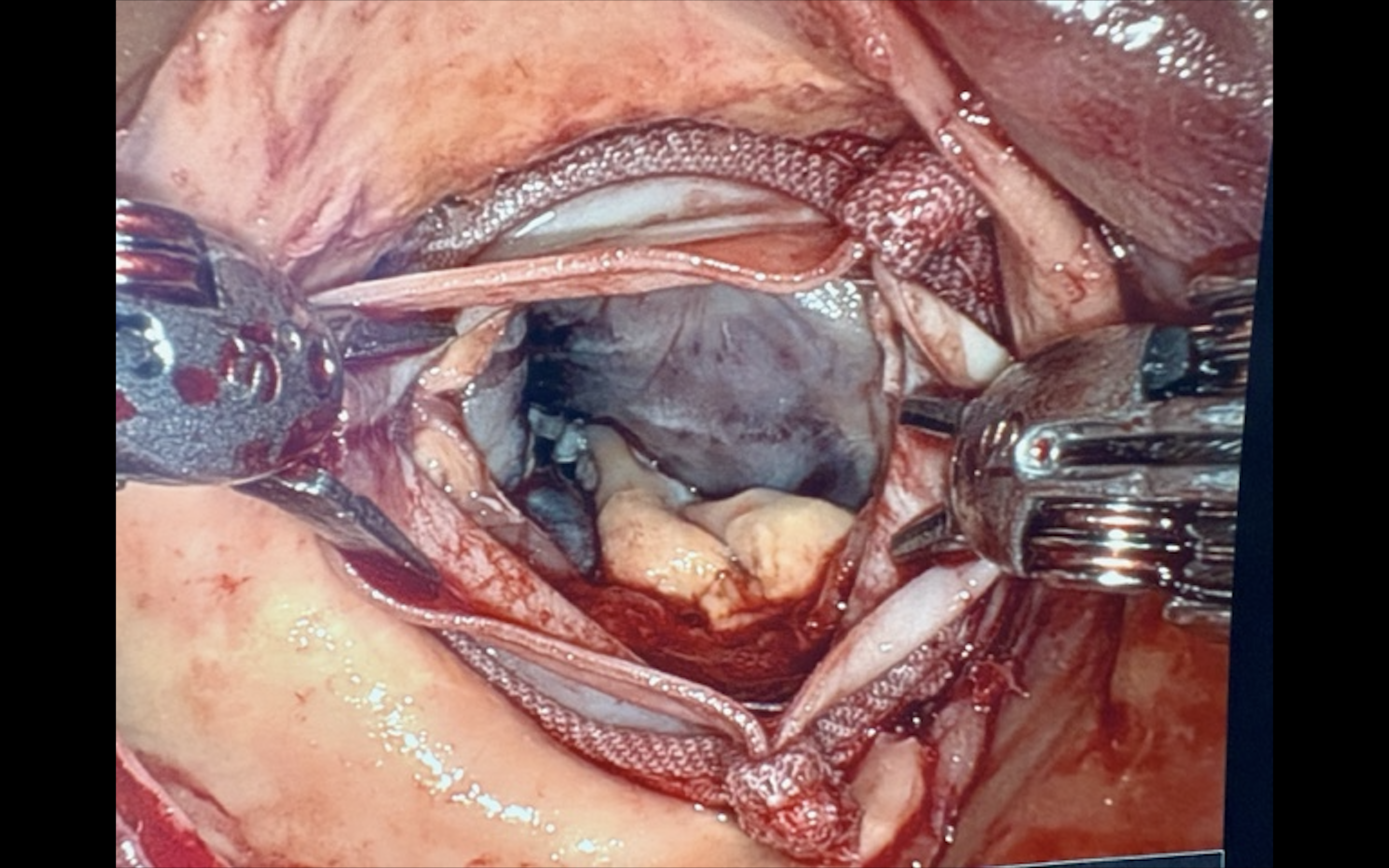
Robotic aortic valve replacement being performed on a patient with severe aortic stenosis. Image courtesy of the WVU Heart and Vascular Institute.
Why perform RAVR over TAVR or SAVR?
According to Badhwar, one of the primary reasons RAVR is gaining popularity is the fact that some cardiologists are simply not comfortable performing TAVR on young or low-risk patients. He is quick to point out that he remains a huge supporter of TAVR when it is the best treatment option. There are many cases, however, where he would much rather see the patient undergo SAVR.
As the debate between TAVR and SAVR continues, Badhwar sees RAVR as “the best of both worlds”—a way to provide high-quality care to a patient who may not necessarily be an ideal candidate for TAVR or SAVR.
“RAVR is not just for low-risk healthy patients," he said. "In fact, robotic cardiac surgery as a whole may often assist in lowering the morbidity for higher risk patients. Let’s say you have a patient who is frail and may not be able to tolerate a sternotomy—but their other risks are lower. That might be a sweet spot for RAVR … and it is important for our cardiology colleagues to know there is another treatment option available that does not involve sternotomy.
The fact that RAVR does not require a sternotomy also makes it a much more attractive treatment option for patients. Patients have preferred TAVR over SAVR for years due to the fact that they do not have to have their chest opened up during the procedure. It saves the body a lot of trauma and helps lead to a much quicker recovery. RAVR, meanwhile, only requires a small incision, potentially helping it stand out to patients as they review their different treatment options.
Another key benefit of RAVR is the fact that operators have the flexibility to address other significant concerns during treatment. Badhwar noted that mitral valve and atrial fibrillation treatments, for example, can be performed during RAVR procedures. Concomitant operations are needed in nearly one in five cases, he added, so this is an advantage that care teams will appreciate time and time again.
Badhwar also pointed to the encouraging outcomes data being seen with RAVR. He is most impressed with the small number of strokes, which continue to be an issue after TAVR.
“The stroke rate for RAVR has been less than 2%,” he said. “That’s because we are seeing every kernel of calcium and aspirating everything meticulously. So, the embolic stroke rate has been negligible across all institutions.”
Learn more about the WVU International RAVR Symposium here. Read a prior interview with Badhwar about RAVR here.

Michael has more than 19 years of experience as a professional writer and editor. He has written at length about cardiology, radiology, artificial intelligence and other key healthcare topics.