
Implantable IVC sensor shows early potential to guide heart failure management
A new-look heart failure monitor that clinicians implant in the inferior vena cava (IVC) to track changes in intravascular fluid volume is both safe and feasible, according to new findings published in JACC: Heart Failure.[1]
It is too early to tell if the device could significantly impact patient outcomes, researchers added, but the sensor did deliver accurate IVC data and showed potential to improve the remote management of heart failure patients.
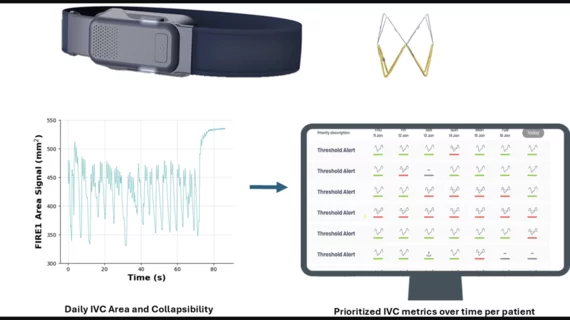
The IVC-based heart failure management technology, now being marketed under the brand name Norm, was developed by in a medical device incubator in California by FIRE1, an Irish medtech company. The goal is to measure changes in a patient’s IVC area and collapsibility, which can help anticipate when heart failure events might occur earlier than other available heart failure monitors. The Norm system includes an implantable sensor, a pusher and loader for delivering that sensor to the IVC, an external hardware unit with a belt and a web application.
“Congestion is a strong predictor of adverse outcomes in patients with heart failure (HF)1,2 but remains difficult to assess and manage,” wrote first author Paul R. Kalra, MD, MA, MB BChir, a cardiologist with Queen Alexandra Hospital in the United Kingdom, and colleagues. “Traditional clinical markers have shown low specificity and sensitivity, and hemodynamic changes suggestive of congestion can be present several days to weeks before manifestation of clinical signs or symptoms, making early recognition a challenge.”
Kalra et al. tracked data from the first 50 patients to receive this device. The mean age was 65 years old and 86% of patients were men. Overall, the study’s primary safety endpoint—procedural success without device- or procedure-related complications—and primary technical endpoint—signal acquisition following implantation and during a clinic visit—were both achieved in 49 of the 50 patients after three months. The one exception was a patient who died before the three-month follow-up for reasons unrelated to the device or the implant procedure.
After six months, the Norm technology was still found to be safe for patients. Another two deaths did occur, but they were once again unrelated to the device or the procedure.
The research team also noted that IVC-derived IVC measurements strongly correlated with CT-derived measurements, confirming the device’s ability to accurately track changes in fluid volume. In addition, after six months, median daily adherence was 96% per patient and more than 7,400 transmissions had been successfully transmitted from the sensor to the cloud.
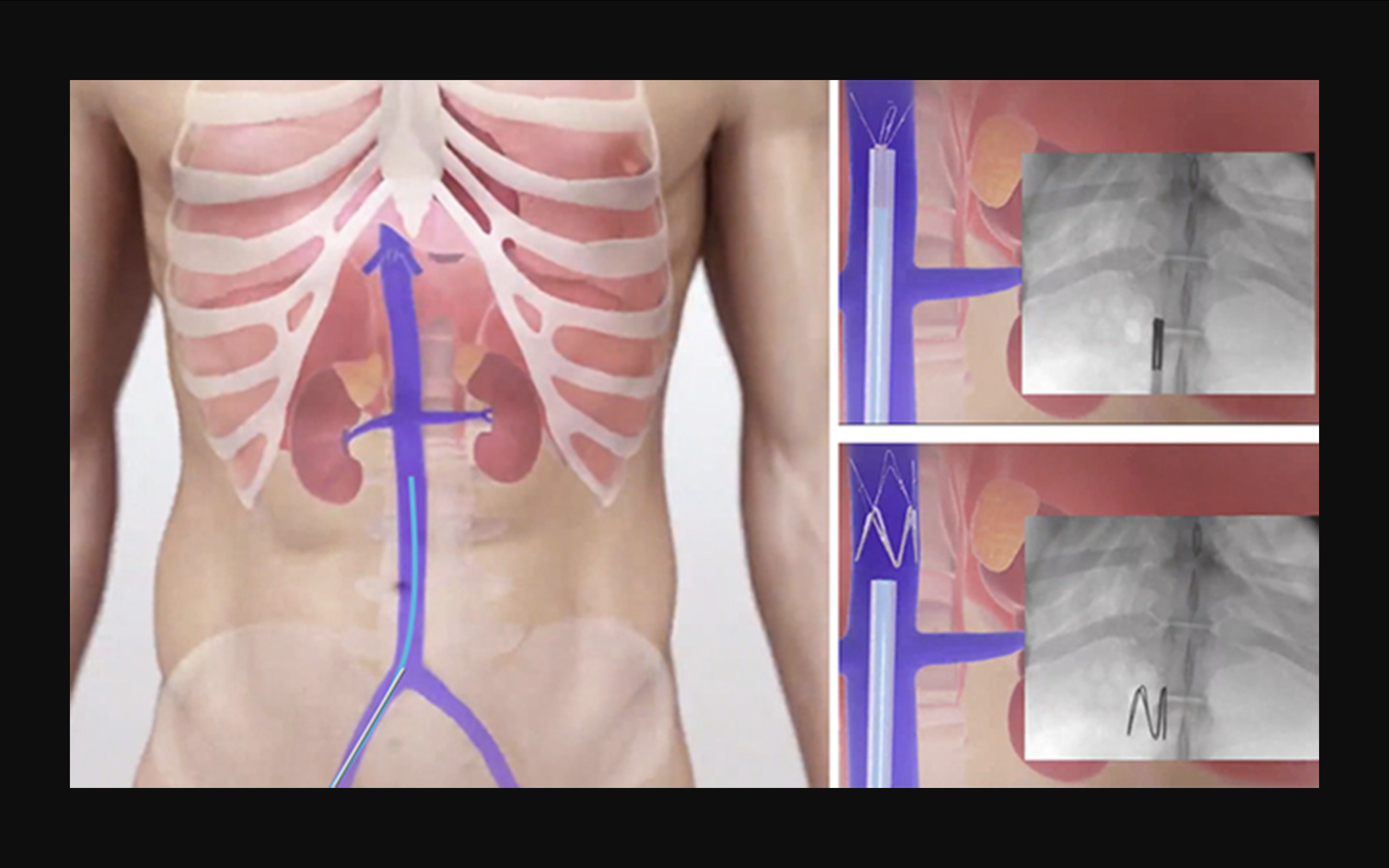
The implantation procedure. Images courtesy of Kalra et al. and JACC: Heart Failure.
At the end of the study, the authors did identify a “significant decrease” in NT-proBNP levels and noted that 12 patients improved from New York Heart Association functional class III symptoms to class II symptoms. On the other hand, no significant differences were seen in body mass index or six-minute walk distances. Use of the technology was also linked to a 80% decrease in heart failure events per patient-year.
“A primary goal of heart failure management is to prevent urgent heart failure readmissions,” the authors wrote. “Being able to detect volume overload (and hypovolemia) earlier than existing technologies is essential to interact sooner with patients to decrease residual heart failure risk. The present findings with the first-in-human experience with the IVC management system show that remote monitoring of IVC dimensions is feasible, with high accuracy and without safety concerns.”
Kalra and colleagues also noted that improvements have already been made to this technology that are designed to improve its effectiveness.
“The next generation of the system will incorporate a mobile application and sensor interaction with direct feedback to the patient,” they wrote. “This will allow comprehensive patient-centered self-management while maintaining minimal physician oversight.”
The team did emphasize that it is still early and more research is required. Multiple studies are already underway, they explained, and once that additional research has been completed and reviewed, they will help provide a better look at this technology’s long-term value.
Click here for the full study.

Michael has more than 19 years of experience as a professional writer and editor. He has written at length about cardiology, radiology, artificial intelligence and other key healthcare topics.