
Many older heart failure patients are alone and vulnerable—what can be done to help?

Older heart failure patients with no immediate family are especially vulnerable, according to a new analysis in the Journal of Cardiac Failure.[1] Additional interventions may be necessary to reach these patients and provide the best care possible.
The study’s authors focused on kinlessness—defined as someone without a living partner or any children—among elderly patients with advanced heart failure. Kinlessness is one of three related social constructs known to impact a person’s physical and mental health. The other two are social isolation and loneliness.
“Social relationships have been associated with health-related quality of life and outcomes in patients with heart failure,” wrote first author Sarah Godfrey, MD, a researcher with the University of Texas Southwestern Medical Center in Dallas, and colleagues. “There are sparse data about kinlessness in this patient population, but both social isolation and loneliness have been independently associated with developing cardiovascular disease, stroke and heart failure by older adults. Once a patient has heart failure, social isolation is further intricately linked with health-related quality of life by impacting mental and physical wellbeing, impeding the ability to follow complex medical regimens and posing challenges in navigating the healthcare system; together, these influences can lead to worse health outcomes.”
Godfrey et al. detailed the many ways kinlessness can impact older heart failure patients. These patients have no one besides clinicians to help them make important decisions, for example, and they lack the support system often needed to follow a doctor’s recommendations. There are clear financial disadvantages as well; when patients have no life partners or children to ask for help, what will they do if the bills for medications and doctor’s visits become too much to handle?
“The higher kinlessness rates in already disadvantaged groups, such as Black, female, disabled, and low-income adults, may exacerbate existing disparities in health outcomes and access to advanced therapies,” the authors added. “Patients with these demographics may struggle with the additional burden of insufficient social support when navigating the complexities of the medical system. For example, kinless adults from rural areas may not have access to transportation to an heart failure specialist outside of their communities. Likewise, kinless adults with low income may not be able to obtain employer-based health insurance from a spouse to cover guideline-directed medical therapy, let alone advanced therapies.”
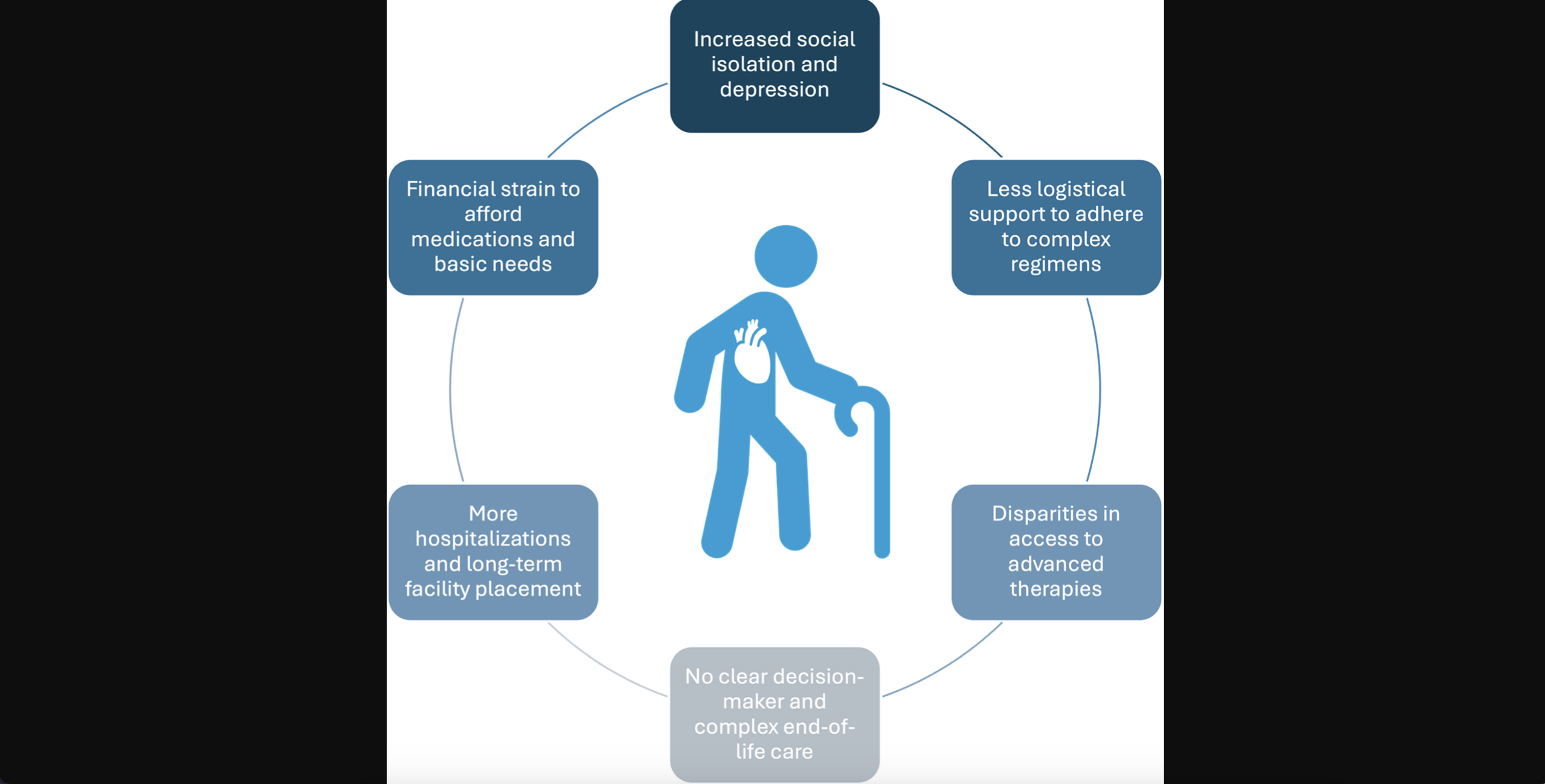
The potential impact of kinlessness on older adults with heart failure. Graphic courtesy of Godfrey et al. and the Journal of Cardiac Failure.
Care requirements and limitations may need to change
What can be done to help reach these patients? First, the authors wrote, adjustments may need to be made to ensure these patients can still be eligible for certain heart treatments. Patients are often denied the use of a left ventricular assist device (LVAD) if they do not have enough social support, for example. Heart transplant candidates are often denied the procedure for the very same reason.
However, LVAD technology has evolved over the years, and heart transplant care has advanced considerably. Telehealth is also now available, making it easier for patients to communicate to their clinicians when necessary. With all of these factors in mind, the group suggested that it is time for some of these requirements to be considered from a different perspective. Denying a patient access to certain technologies or procedures because they find themselves in a vulnerable social state may not be the best path forward.
Godfrey and colleagues also noted that older adults with no immediate family may still have many friends who could provide support when needed. In addition, social workers can provide assistance in some cases by helping patients find support communities or connecting them with other helpful resources.
Innovation in how older adults live
True innovation is also needed to improve care for these patients—and one area where there is an opportunity for such change is in the way these patients live. The study’s authors noted that one trend starting to pick up steam is “alternative group-living arrangements” among older adults.
“Separate from long-term care facilities, movements to have older adults ‘age in place’ in the community have adopted three models of alternative housing: shared housing, cohousing and villages,” the authors wrote. “In shared housing situations, an older adult rents part of her/his house to a younger adult at a discount in exchange for assistance with household chores, transportation and other caregiver support roles. Matchmaking services to facilitate shared housing arrangements are growing across the United States. Cohousing involves multiple older adults purchasing a housing complex for residents to live together and determine residential norms and rules collectively … Adapted from European models, the village movement involves groups of older adults living in a neighborhood and who pay dues to a ‘village,’ which provides a range of support services, including help with household tasks, recreational and social activities and transportation.”
The power of smartphone apps
The group also looked at innovation on the technological side of things, highlighting the need for smartphone applications that help older patients manage their health. Such apps could help LVAD or heart transplant patients interact with their physicians whenever needed and track their symptoms.
“Although this is a complex and multifaceted public health challenge, creative solutions are needed to ensure that patients are not denied appropriate care because they do not have traditional kin,” the authors wrote.
Click here to read the full study.

Michael has more than 19 years of experience as a professional writer and editor. He has written at length about cardiology, radiology, artificial intelligence and other key healthcare topics.