
‘Practice-changing’ interventional cardiology research grabs ACC.26 spotlight
The second day of ACC.26, the American College of Cardiology’s annual conference in New Orleans, opened up with a series of highly anticipated interventional cardiology studies.
In fact, Jane Leopold, MD, director of the Women's Interventional Cardiology Health Initiative at Brigham and Women’s Hospital and deputy editor of The New England Journal of Medicine, described all four presentations as “exceptional, practice-changing studies.”
Elective LV unloading in high-risk PCI
Divaka Perera, MD, professor of cardiology at King’s College London, kicked things off by presenting data from CHIP-BCIS3, his team’s analysis of elective left ventricular unloading with a microaxial flow pump for certain high-risk percutaneous coronary intervention (PCI) procedures.
The group enrolled 300 patients with a mean age of 73 years old. While 83% of patients were male, 85% were white. Patients were randomized to either undergo PCI with a microaxial flow pump—Johnson & Johnson MedTech’s Impella CP heart pump—or undergo traditional PCI. While these were high-risk patients, they were still largely stabilized at the time of treatment and undergoing a planned PCI procedure.
Overall, researchers found that elective LV unloading was not associated with any significant benefits in terms of major clinical outcomes after one year. Some smaller benefits were seen in specific instances, but they came at the cost of an increased risk of vascular complications.
“This was surprising because the whole premise of LV unloading was that it protects the heart,” Perera said. “But we found that patients assigned to LV unloading had more damage to the left ventricle than those assigned to standard care.”
He added that he and his team “found an excess of death due to cardiovascular causes in patients who are assigned to have a microaxial flow pump.” They hope to share more details about this finding in the near future.
Roxana Mehran, MD, a professor at the Icahn School of Medicine at Mount Sinai and leading voice in the field of interventional cardiology, was on the ACC.26 stage as a panelist when Perera shared these data. She thanks Perera for his team’s “very, very important trial” and provided additional context about his findings.
“This is an important and long-awaited randomized clinical trial that addresses a question that many of us face daily in the cath lab,” she said. “Over the last decade, we have increasingly adopted mechanical circulatory support for high-risk PCI, particularly the microaxial flow pumps, largely driven by physiological rationale and observational experience. The concept is intuitive. Unloading the ventricle should improve hemodynamic stability, allow more complete revascularization and ultimately improve outcomes. However, until now, we have lacked definitive randomized evidence against the true contemporary standard of care.”
Mehran said current industry guidelines have remained cautious about the use of microaxial flow pumps during high-risk PCI due to a lack of conclusive research. This trial helps finally provide answers, though she did emphasize that certain patient groups—including those in cardiogenic shock—were excluded.
“This distinction is essential because it places it in a very, very different biological and clinical context compared to the previous trial, DanGer Shock, where unloading is tested in patients with active infarct-related shock,” she explained.
These findings were simultaneously published in The New England Journal of Medicine.[1]
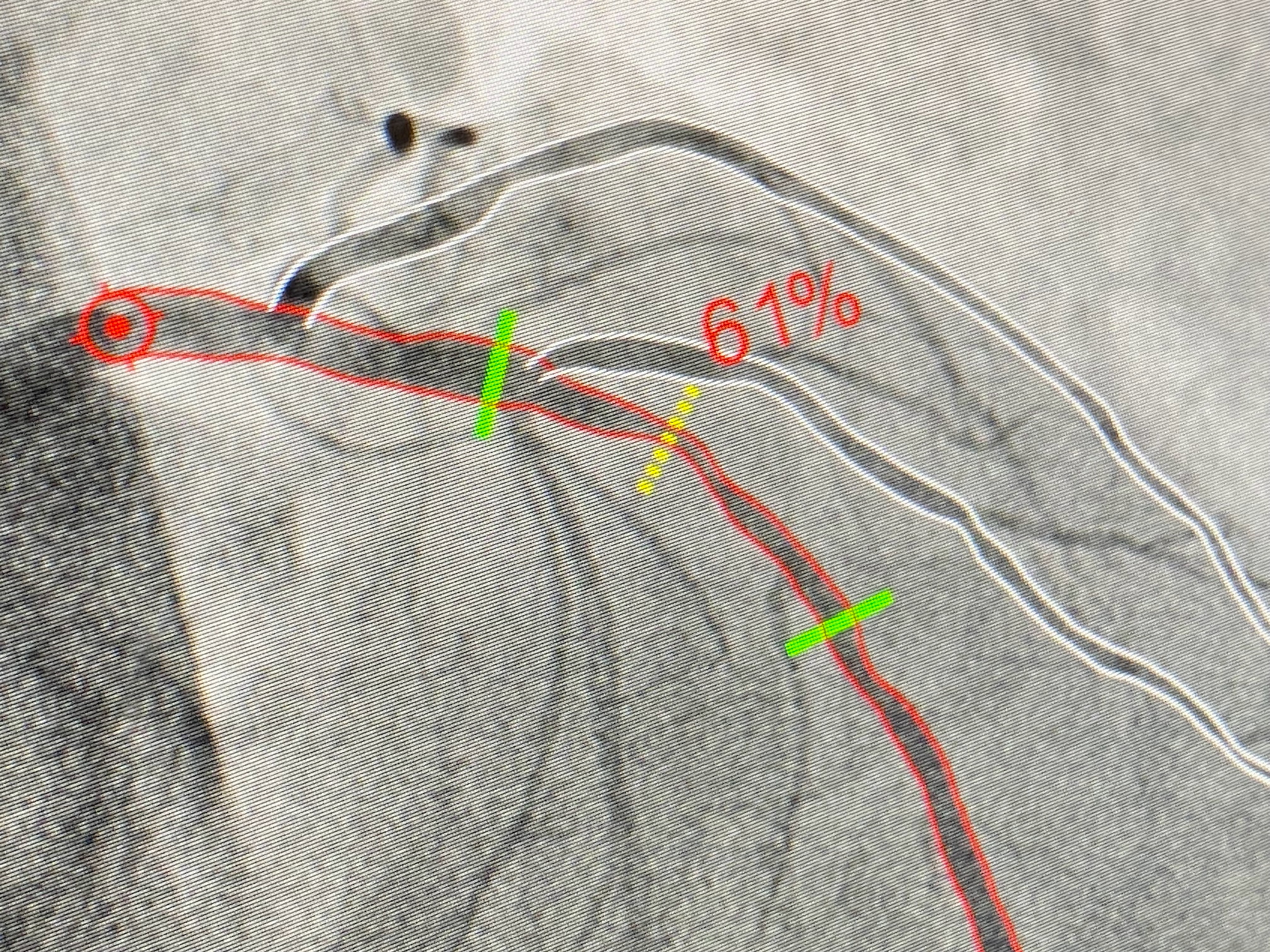
The CathWorks FFRAngio technology in action. Photo taken during TCT 2023.
CathWorks technology put to the test
Ajay J. Kirtane, MD, an interventional cardiologist at NewYork-Presbyterian/Columbia University Irving Medical, presented findings from ALL-RISE, his team’s look at the artificial intelligence-enabled FFRangio technology developed by CathWorks.
FFRangio received U.S. Food and Drug Administration clearance in 2018. Kirtane et al. compared the advanced AI technology with invasive wire-based assessments of patients with suspected coronary artery disease. Their research included nearly 2,000 patients with a mean age of 68 years old. Patients were recruited from the United States, Israel, Japan, Switzerland and the U.K. While 75% of these patients were men, 60% were white.
Patients were randomized to undergo an evaluation with either FFRangio or a wire-based measurements. The findings from those assessments were then used to help cardiologists determine if they would perform PCI.
Overall, the two treatments were associated with similar results. The study’s primary outcome—the rate of one-year major adverse cardiovascular events—occurred in 6.9% of patients treated with the CathWorks technology and 7.1% of patients assessed with wire-based techniques. Procedure times and fluoroscopy times were also significantly shorter for patients treated with FFRangio.
“These data support the routine use of FFRangio to guide treatment of intermediate lesions in the cath lab with a simplified workflow over the current standard of pressure wire-based assessment,” Kirtane concluded. “We hope that this will facilitate an increased use of coronary physiology concordant with guidelines.”
David Moliterno, MD, a professor of medicine at the University of Kentucky and editor-in-chief of JACC: Cardiovascular Interventions, was on hand for Kirtane’s presentation.
“I think this is what we've been looking for,” he said. “I think this is a call—no pun intended—that we should all rise in the cath lab and use physiology more. I was also happy to see that roughly half the patients had intravascular imaging. I think this is a really good cutting-edge study.”
Moliterno did note that more patients were chosen to undergo PCI in the group treated with FFRangio. Is it possible, he wondered, that the benefits in procedure times are canceled out by the fact that more patients are undergoing treatment?
“I'm certainly not advocating for doing more PCIs,” Kirtane said. “I think that one of the benefits and beauties of using physiology is that you actually don't do unnecessary PCIs.”
These findings were simultaneously published in The New England Journal of Medicine.[2] The study comes at an exciting time for CathWorks. Back in February, Medtronic agreed to acquire the company for up to $585 million.
“The ALL-RISE data affirm our confidence in FFRangio's transformative impact on the diagnosis and treatment of coronary artery disease,” Jason Weidman, senior vice president and president of Medtronic’s coronary and renal denervation business, said in a statement. “We are excited for the future with CathWorks and believe FFRangio is poised to become a new standard worldwide.”
Another home run for noninvasive FFR
Joost Daemen, MD, PhD, associate professor at the Erasmus University Medical Center in Rotterdam, Netherlands, presented data from a related study just minutes later. For the FAST-III trial, his team compared the vessel FFR (vFFR) technology developed by Pie Medical Imaging with more traditional, wire-based FFR measurements.
vFFR builds 3D reconstructions of a patient’s coronary artery using two routine angiograms. In addition to providing care teams with a noninvasive treatment option, the technology was also designed to improve workflows by speeding up procedure times.
Daemen et al. tracked data from more than 2,000 patients treated at one of 37 European facilities. The mean age was 67 years old and 75.7% were men. Patients were randomized to either undergo vFFR-guided revascularization or more traditional FFR-guided revascularization.
Overall, the study’s primary outcome—a composite of death from any cause, myocardial infarction or revascularization after one year—was the same for both groups. Endpoint events occurred in 7.5% of vFFR patients and 7.5% of traditional FFR patients.
William Fearon, MD, a professor with Stanford Medicine and experienced research of FFR technologies, praised FAST-III as a “well-conducted, impactful trial.”
“I think based on these data and the data Dr. Kirtane presented on ALL-RISE, we can conclude that angiography-derived physiology is here to stay,” Fearon said.
He added that some studies in recent years have concerned cardiologists about these technologies because they were unable to confirm noninferiority. Now, however, two studies presented over the course of just a few minutes both highlighted just how impactful these systems can be.
These findings should make a significant impact on heart patients for many years to come, Fearon noted, including improved care and better patient outcomes.
"FAST III marks a defining moment. It confirms angiography-based physiology is non-inferior to conventional pressure wire-based physiology," Bas Kuppens, CEO at Pie Medical Imaging, said in a company statement highlighting the positive data. "Additionally, it has demonstrated benefits for care givers and patients by requiring less dose, less contrast agent, and reducing procedure lead time."
These findings were simultaneously published in The New England Journal of Medicine.[3]
Confirming the benefits of CTO PCI
John Davies, MRCP, PhD, a consultant interventional cardiologist at the Essex Cardiothoracic Center presented new data on the benefits chronic total occlusion (CTO) PCI.
Care teams regularly turn to CTO PCI to help reduce the risk of angina and improve a patient’s quality of life. However, it remained unclear whether these patients were truly benefiting or if a placebo effect was responsible for many of the reported improvements.
For the ORBITA-CTO trial, Davies et al. review data from 50 patients with a median age of 64 years old. Nearly three in four of these patients were men. All patients had a completely blocked coronary that had been present for at least three months in addition to angina symptoms, even after being prescribed anti-anginal medications. Patients were randomized to either undergo CTO PCI or receive a placebo procedure.
Overall, patients in the treatment group were associated with statistically significant improvements in quality-of-life scores and a reduced risk of angina. No deaths or myocardial infarctions occurred.
“These results provide hope for both patients with CTO and their doctors that angioplasty with stenting can be successful and can result in reduced angina pain and better quality of life,” Davies said.
J. Dawn Abbott, MD, director of interventional cardiology and the cardiac cath labs at Brown University Health Cardiovascular Institute, congratulated Davies and his team for presenting “a truly impressive trial.”
It may have been a small study, she added, but it did help highlight the continued safety of CTO PCI in addition to consistent quality-of-life improvements.
“The relative benefit of PCI was dramatic,” she said.
These findings were simultaneously published in JACC.[4]

Michael has more than 19 years of experience as a professional writer and editor. He has written at length about cardiology, radiology, artificial intelligence and other key healthcare topics.