
Q&A: Interventional cardiologist details key breakthroughs in tricuspid valve replacement and repair

2024 has been a banner year for structural heart treatments, especially those focused on the tricuspid valve. In February, for example, Edwards Lifesciences made history when its Evoque transcatheter tricuspid valve replacement (TTVR) system became the first device of its kind to gain U.S. Food and Drug Administration (FDA) approval for treating tricuspid regurgitation (TR). Two months later, Abbott’s TriClip transcatheter edge-to-edge repair (TEER) system also gained FDA approval for the treatment of TR.
Just like that, interventional cardiologists went from having no FDA-approved treatments for TR to two—and many other similar devices are in development. What should care teams take away from these big breakthroughs in tricuspid care? How do cardiologists choose between tricuspid repair and replacement?
To explore those questions, and many more, Cardiovascular Business spoke with Andrew Rassi, MD, an cardiologist with Kaiser Permanente’s San Francisco Medical Center. Rassi specializes in interventional treatments and presented a session about tricuspid valve trends at ACC.24, the American College of Cardiology’s annual meeting in Atlanta.
Cardiovascular Business: Can you provide background on the last few years in tricuspid valve repair and replacement? How have interventional cardiologists viewed this topic with no FDA-approved devices available until just a few months ago?
Andrew Rassi, MD: Until the recent FDA approvals, we have seen an evolution in the way cardiologists and interventional cardiologists have managed patients with tricuspid regurgitation (TR). Previously, these patients were managed with diuretics for symptom improvement, but surgical treatment was only reserved for very healthy patients, or those already undergoing left sided valve surgery. That accounts for a very small proportion of patients with this disease process. Over the last five to 10 years, with the advent of transcatheter options in various phases of development, we have seen interventional cardiologists start to offer percutaneous treatment options, initially through off-label use of FDA-approved devices and then in the context of clinical trials with devices that were designed to address the tricuspid valve.

Andrew Rassi, MD
What were your thoughts when the Evoque TTVR system from Edwards gained FDA approval back in February?
Our site is part of the TRISCEND II pivotal trial, so I will limit my responses to data that is available publicly given that the final results of the trial are yet to be presented.
For the first time, we now have an FDA-approved device that is dedicated to the tricuspid valve and essentially eliminates TR for almost all patients who are eligible. There are many patients who will not be eligible for this device even with recent FDA approval due to anatomic factors as well as patient factors such as inability to tolerate oral anticoagulation. While we know that patients note improved quality of life metrics and have improvements in their walk scores, we are still learning which patients derive symptomatic benefit from treatment of their TR and if that treatment will result in an improvement in clinical outcomes such as reductions in heart failure hospitalizations or improved mortality.
The fact that this device was approved by the FDA without published data and without the final outcomes of the study speak to the unmet clinical need for any potential treatment for this group of patients, who previously had little to no options.
What about the TriClip TEER device? Was it surprising to see the two devices approved in a span of just a few months?
Unlike the Evoque, TriClip was approved after reaching the primary endpoint of its trial with a published data set. The procedure is very safe and has a low rate of major adverse events. It is also an effective device in reducing the amount of TR. Although no direct comparisons between the two FDA-approved devices exist, in general, we see a smaller effect on the degree of residual TR with TriClip than with Evoque. We do not yet know how much TR reduction is necessary to see clinical improvement with any of these devices.
As the field moves forward, interventional cardiologists are going to have multiple devices available with varying treatment strategies and are going to have to weigh the relative effectiveness and safety of each device when making determinations about the right device for each patient.
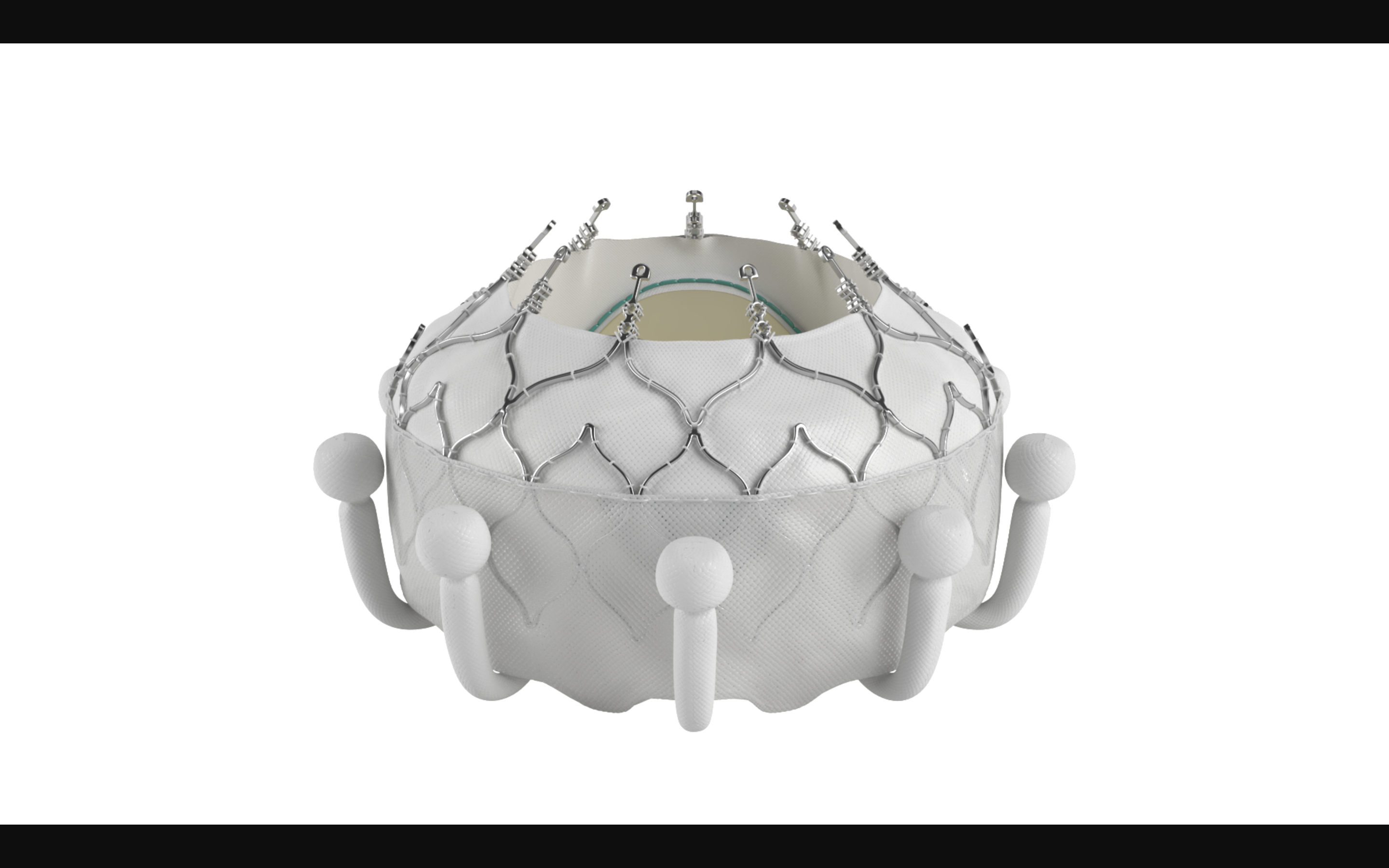
The Evoque TTVR device. Image courtesy of Edwards Lifesciences.
How do the Evoque and TriClip approvals change the landscape for any similar devices being pushed toward FDA approval?
It is a blessing to now have two FDA-approved devices that will offer therapeutic options to patients who previously didn’t have many. However, on the flip side, approving devices prior to reaching the primary endpoint or with symptomatic improvement but a less compelling hard endpoint may lead to certain challenges. While the creation of a new field of interventional cardiology to treat TR will certainly inject more investment into the space, having two FDA-approved devices also changes the landscape for devices that are already in development and will have implications on the way they are tested and how quickly those other devices may ultimately come to market. Any subsequent trials will now have to compare data to an FDA-approved device rather than to medical therapy alone.
What other tricuspid valve repair or replacement devices do you have your eyes on right now?
There are more devices in clinical trials for the tricuspid valve at this time than we could possibly discuss. Some are farther along than others and only a few have had successful implants in humans to date. The number of devices being studied speaks to the unmet clinical need that will only be partially answered with the two FDA-approved devices.
We know that many patients will need unique solutions to overcome limitations of the other devices, such as the pacemaker rate, the risk of single leaflet detachment or anatomic exclusions that prevent implant. These devices can be grouped into a few categories:
• Replacement devices (orthotopic and heterotopic)
• Leaflet coaptation devices
• Annular repair devices
Similarly, the concept of lifetime management will eventually be an important concept—we know that implanting some devices as a first therapy will close the door to subsequent transcatheter treatment options. Therefore, the devices I’m most excited about are those that will allow us to either remove prior devices or allow us to treat in spite of the presence of a prior device.
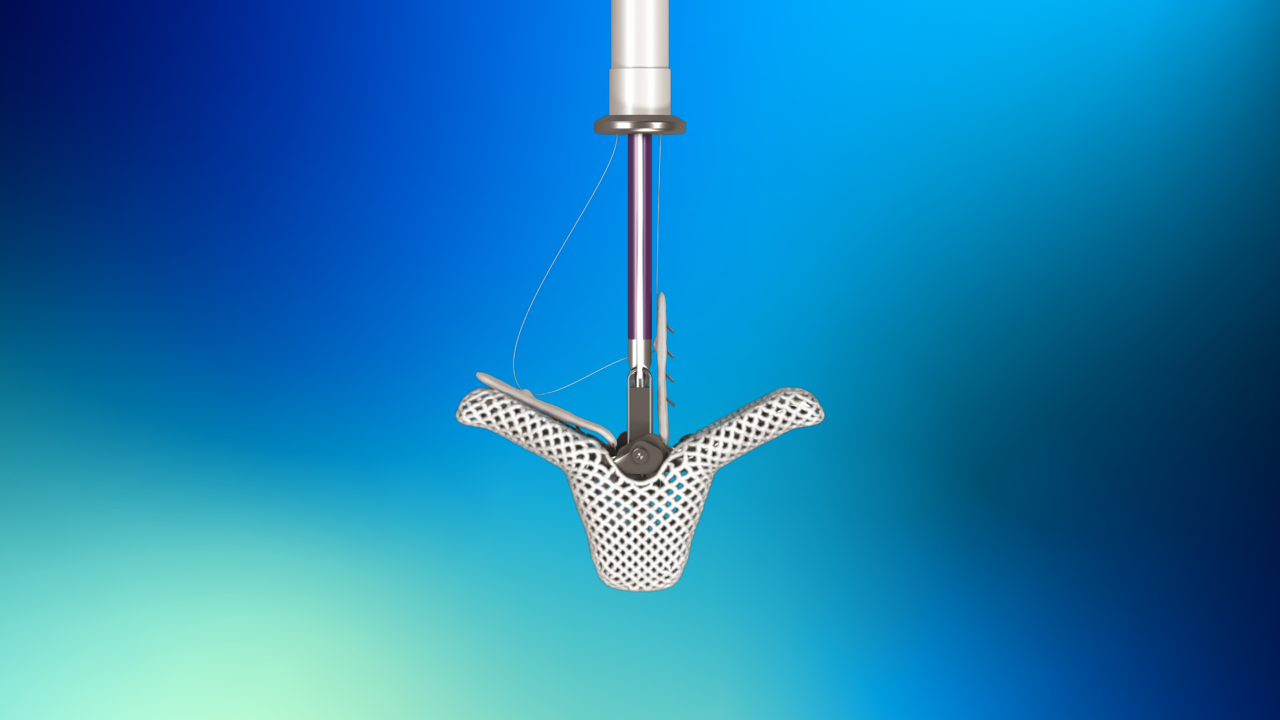
The TriClip T-TEER device. Image courtesy of Abbott.
How should care teams handle the decision of tricuspid repair vs replacement?
At this stage, guidelines continue to recommend surgical repair/replacement for patients already undergoing left sided valvular surgery. However, for those who are not surgical candidates, there are no direct comparisons between repair/replacement at this time. The relative reduction in TR compared to the relative risk for each device will need to be assessed.
Similarly, each patient’s anatomy might be better suited for one strategy than the other. An ongoing study of patient subsets who derive the most clinical benefit from each device will be an important factor in making this determination. One thing is for certain: although we know more than we did five years ago about TR and treatment options, we currently know less as a medical community than we’d like to know. I have every confidence that when we look back in the next five or 10 years, the field will look very different.
You mentioned the challenges associated with the right ventricle during your presentation at ACC.24. Can you go into a bit more detail about this?
Right ventricular (RV) dysfunction can best be thought of as a downstream effect of severe TR, but it is also a contributing factor to its development. It can be both “the chicken or the egg” and will certainly have implications on who benefits most from procedures designed to treat TR. Given that patients come to us at various stages along the continuum of TR and RV dysfunction, we need to better understand in whom the RV will recover following TR treatment and in whom the RV is too far gone and may continue to plague patients with worse outcomes despite successful treatment of their TR.

Michael has more than 19 years of experience as a professional writer and editor. He has written at length about cardiology, radiology, artificial intelligence and other key healthcare topics.