
New LAAO guidelines: 6 key takeaways for interventional cardiologists and electrophysiologists
The Society for Cardiovascular Angiography and Interventions (SCAI) and Heart Rhythm Society (HRS) have published new evidence-based guidelines designed to bring more consistency to the way left atrial appendage occlusion (LAAO) procedures are planned and performed.
The guidelines are available in full in both JSCAI and Heart Rhythm.[1, 2]
In 2023, SCAI and HRS worked together on an expert consensus statement about transcatheter left atrial appendage closure. However, pointing to a “considerable variation in real-world clinical practice” that remains to this day, the groups wanted to publish additional guidelines that emphasized the importance of doing the right thing at the right time for each patient.
“These guidelines are intended to help clinicians and patients make decisions about LAAO, including pre-, intra-, and post-procedural interventions and their alternatives,” wrote Andrew M. Goldsweig, MD, MS, a cardiologist with the University of Massachusetts-Baystate, and the rest of the writing group. “In addition, these guidelines should also serve to guide policy, education, and advocacy while highlighting knowledge gaps for future research. These guidelines should not be construed as a standard of care. Clinicians should tailor decisions according to the unique circumstances of each patient, ideally through a collaborative approach that considers the patient’s values and preferences. The decision-making process may be influenced by clinical settings, local resources, institutional policies and availability of treatments, technologies or providers.”
6 key takeaways from SCAI and HRS
1. When patients with nonvalvular atrial fibrillation (NVAF) are not suitable for oral anticoagulation (OAC), LAAO is recommended over no therapy at all.
“Many patients with contraindications to OAC would reasonably choose to reduce their stroke risk by selecting LAAO over no therapy,” the authors wrote. “Patients who value avoiding possible procedure-related adverse events more than a possible reduction in risk of stroke would reasonably choose no therapy. Clinicians should discuss with patients the procedural risk of LAAO vs the ongoing risk of thromboembolic events associated with no treatment.”
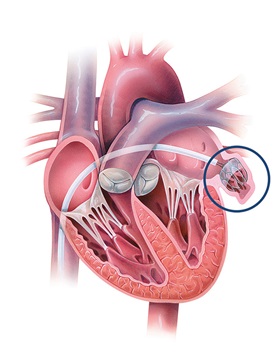
Illustration of a left atrial appendage occlusion (LAAO) procedure using a Watchman device. Image courtesy of Johns Hopkins Medicine.
2. When patients with NVAF are suitable for OAC, LAAO may still be the preferred treatment strategy in certain cases. For example, if there is an elevated bleeding risk, prior bleeding complications or the patient strongly opposes taking long-term anticoagulation, it may make more sense to consider LAAO over OAC.
3. When patients with NVAF are undergoing LAAO, transesophageal echocardiography (TEE) or cardiac CT are recommended prior to the procedure and intracardiac echocardiography (ICE) or TEE are recommended during the procedure.
4. Following LAAO, either OAC or dual antiplatelet therapy (DAPT) are recommended.
“Patients with more significant contraindications to OAC (eg, severe bleeding history or risk) would reasonably select DAPT,” the authors wrote.
5. Post-procedural TEE or cardiac CT are recommended to review the procedure’s effectiveness.
6. In patients with a device-related thrombus, OAC is recommended. Additional research is still required when it comes to determining the optimal duration and timing of OAC for these patients.
The team behind these guidelines also emphasized that LAAO is typically an elective procedure, so care quality must remain high and complication rates must remain low. They pointed to the NCDR LAAO Registry as a “valuable resource” for care teams looking to improve patient outcomes and provide consistent care to these patients.

Michael has more than 19 years of experience as a professional writer and editor. He has written at length about cardiology, radiology, artificial intelligence and other key healthcare topics.