
Cardiologists make history, use new robotic imaging system for first time

Robotic transesophageal echocardiography (TEE) procedures are both safe and feasible, according to a new first-in-human study published in JACC: Cardiovascular Imaging.[1] These procedures could potentially improve TEE in numerous ways in addition to improving patient access to these important imaging procedures.
“Despite its critical role, the interventional echocardiography (IE) specialty has only recently gained recognition, marked by standardized training curricula developed by the American and European societies to ensure safety and effectiveness in structural heart disease (SHD) interventions,” wrote first author Jury Schewel, MD, an interventional cardiologist and imaging specialist with Marien Hospital in Germany, and colleagues. “However, IE specialists face significant challenges, including physical proximity to radiation sources during fluoroscopy-guided procedures, resulting in radiation exposure levels up to 10 times higher than among interventional cardiologists. Additional challenges include achieving consistent high-quality imaging, preventing esophageal and gastric injury, and addressing a shortage of qualified echocardiographers willing to meet the growing demand for SHD interventions.”
ROB’E, a German startup, has developed a new remote-controlled robotic (RCR) system with these challenges in mind. Users are able to remotely manipulate TEE probes, performing precise movements and even saving specific positions so they can be duplicated as needed.
Schewel et al. shared their first-in-human experience using this RCR system on five patients. Three patients presented with severe heart valve disease, and the other two presented for patent foramen ovale screening after a stroke. All patients underwent a standard manual TEE followed by an RCR-guided TEE to evaluate the technology’s safety and feasibility.
The manual TEEs included five standard views and the average time was 8 minutes and 49 seconds. The TEE probe was then installed into the RCR system and the echocardiographer repeated the exam, acquiring the same five views in an average time of 12 minutes and 10 seconds. Each patient was evaluated for any signs of injury after the RCR-guided TEE had been performed.
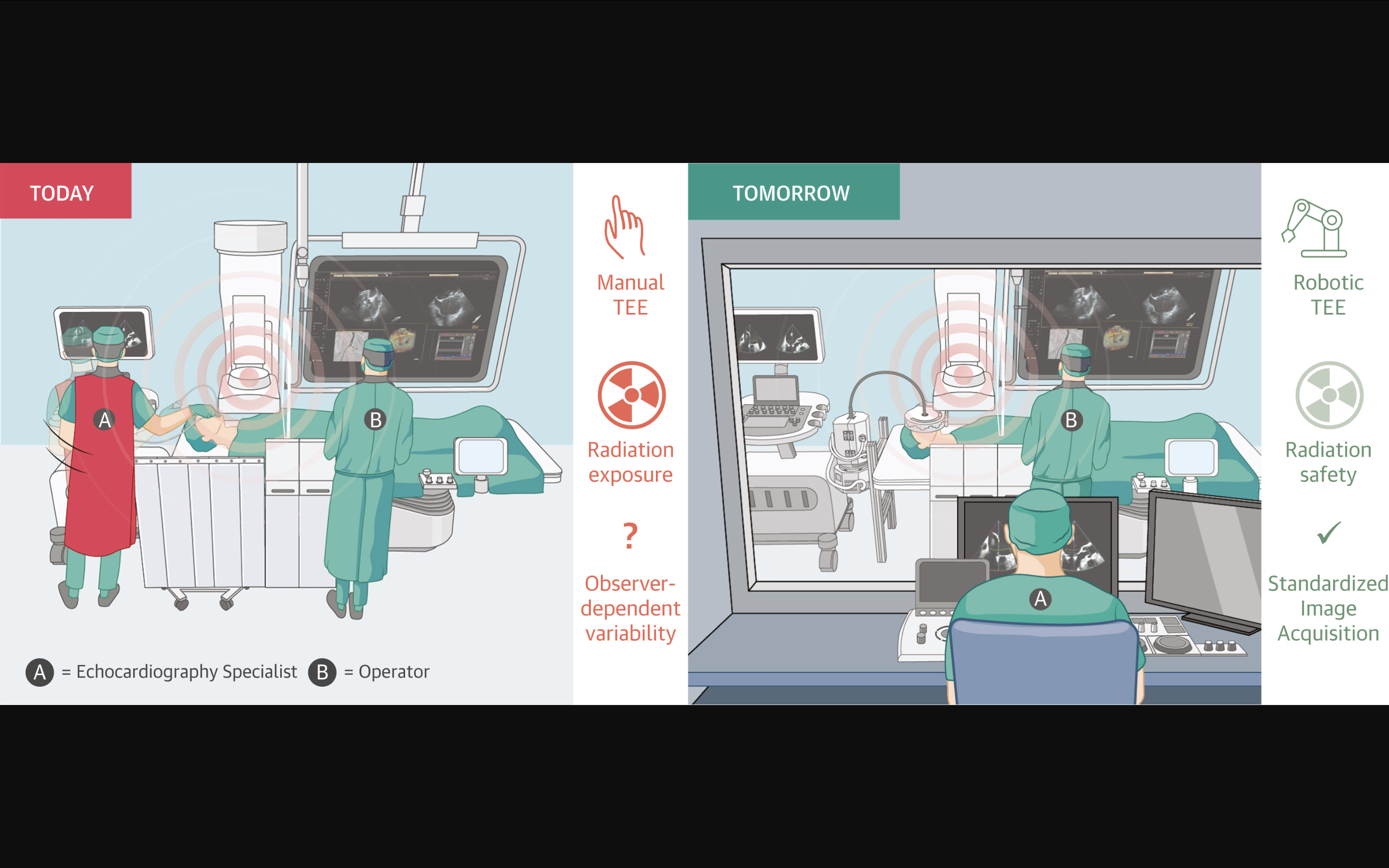
Current setup in an operating room with an X-ray system and an echocardiographic machine operated by an echocardiographer (A) to visualize cardiac structures so that the surgeon (B) can position the device correctly. Tomorrow: The echocardiographer (A) operates remotely from outside the operating room using a control panel, maneuvering the probe installed in the robotic system for safer and more precise imaging guidance. Graphic and caption courtesy of Schewel et al. and JACC: Cardiovascular Imaging.
Overall, the group reported, this new technology successfully performed all necessary movements and acquired all necessary views. The clinical success rate and technical success rate were both 100%. No procedure-related complications were reported. In addition, the RCR system delivered 75% reproducibility of the stored views, and the average switching time was 16.28 seconds.
“This is the first successful trial worldwide demonstrating the use of an RCR TEE system in humans,” the authors wrote. “The study demonstrates the feasibility of performing TEE imaging with the RCR system, achieving precise probe manipulation with high consistency. This innovative technology offers a promising solution to address the challenges and limitations of manual TEE imaging, particularly in the demanding field of IE.”
The group noted that this system should reduce radiation exposure “to near zero” while also improving the ergonomics of interventional echocardiographers. It should also make these procedures safer, “potentially making the field more accessible and gender inclusive.”
“Access to SHD therapies remains limited in underserved areas, partly because of a shortage of IE specialists,” the authors added. “An automated RCR TEE system could support these challenges, while complementing other technologies, such as artificial intelligence–supported handheld ultrasound for earlier detection and diagnosis. Moreover, RCR systems may shorten procedural times, reduce reinterventions, and offer long-term cost savings for healthcare systems, helping address disparities in SHD care.”
Co-authors for this first-in-human analysis were Rebecca T. Hahn, MD, director of interventional echocardiography the Columbia Structural Heart and Valve Center and a known leader in cardiovascular imaging; Martin B. Leon, MD, an interventional cardiologist with Columbia University Irving Medical Center and founder of the Cardiovascular Research Foundation; and Dimitry Schewel, MD, PhD, head of structural heart disease therapy with Marien Hospital.
All study authors either hold leadership positions with ROB’E or serve on its advisory board.
Click here to read the full study in JACC: Cardiovascular Imaging, an American College of Cardiology journal.

Michael has more than 19 years of experience as a professional writer and editor. He has written at length about cardiology, radiology, artificial intelligence and other key healthcare topics.