
ASNC says PET is now the preferred nuclear imaging test for CAD

The American Society of Nuclear Cardiology (ASNC) has shared its official answer to a decades-long debate over which cardiac nuclear imaging modality is the best for evaluating heart patients. In a new position statement, the group officially recommended that cardiac positron emission tomography (PET), if available, be used to evaluate all patients with suspected coronary artery disease (CAD) who are candidates for myocardial perfusion imaging (MPI). The statement was published in full in the Journal of Nuclear Cardiology.[1]
This is a significant moment in the world of nuclear imaging. The statement's authors include six former ASNC presidents, and it codifies the group's push in the past several years to get hospitals to buy more PET systems.
The statement emphasizes extensive scientific research, worldwide clinical experience, and the latest multisocietal cardiology guidelines affirming cardiac PET’s high diagnostic accuracy, powerful risk stratification and low radiation exposure. ASNC has also highlighted PET's expanded ability to assess coronary microvascular disease, myocardial viability, cardiac sarcoidosis, cardiac amyloidosis and infection.
“Based on the massive amount of clinical and scientific information now available and the latest U.S. and European guidelines, ASNC now recommends that PET MPI with myocardial blood flow (MBF), if available, should be the preferred modality for patients who meet criteria for MPI,” ASNC Past President Timothy Bateman, MD, the lead author of the position statement, said in a press release. “There are no clinical scenarios or patient subgroups where cardiac PET with myocardial blood flow should be excluded.”
Single photon emission computed tomography (SPECT) has been the workhorse nuclear imaging modality for cardiac perfusion studies since the 1970s. The introduction of PET in the 1990s brought improved image quality, and hybrid PET-CT systems with CT attenuation correction further pushed the needle in favor of PET. But barriers of greater cost, expensive radiotracers and low access to PET systems limited its wider use.
While there have been incremental technology improvements in SPECT technology with digital detectors, AI attenuation correction software and SPECT-CT, PET has maintained a lead in image quality. It also provides added value with its myocardial blood flow (MBF) assessments, especially for the evaluation of microvascular disease, which is not detectable on SPECT.
The position statement also detailed the clinical advantages of cardiac PET MPI, including increased diagnostic accuracy, risk stratification, reproducible myocardial blood flow quantification and more rapid exam times. The CT component of PET-CT also adds anatomical information and the ability to add on CT calcium scoring on the same exam.
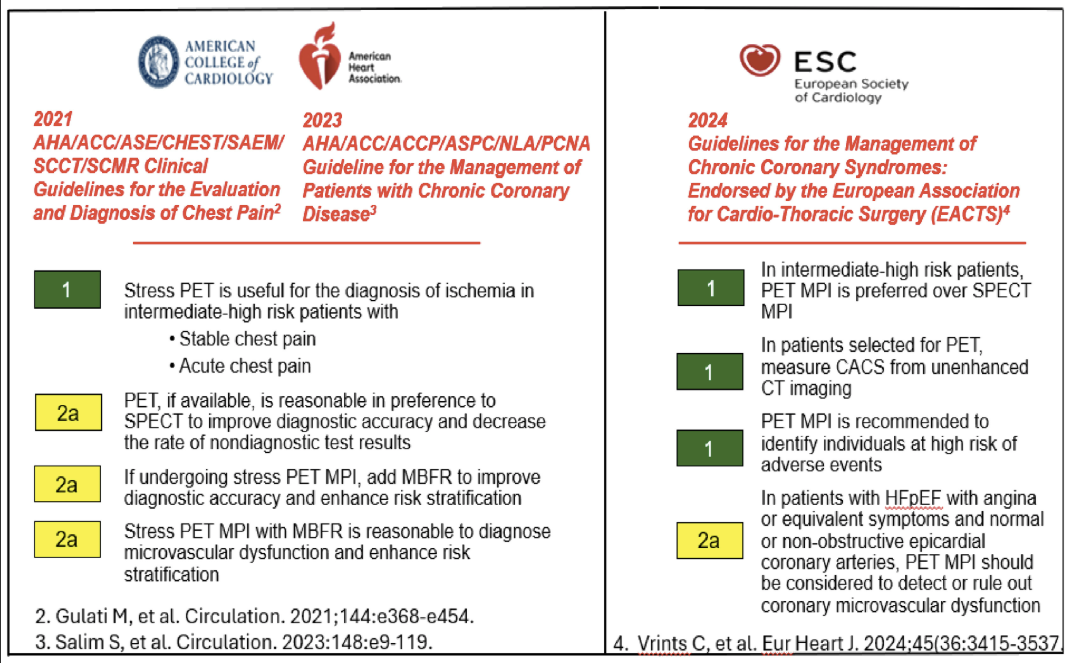
Figure 1 from the clinical statement, showing recommendations for PET MPI in major U.S. and European cardiology guidelines. The green boxes show class 1 recommendation and yellow boxes are for class 2a recommendations.
ASNC statement could change insurance coverage for PET
ASNC had economic reasons for developing this statement as well. It is aimed at eliminating insurance prior authorization denials for the use of PET based on previous descriptions for which patients are best for PET exams. This stems from ASNC’s 2016 recommendations, which listed specific scenarios where PET MPI should be favored. The society said those limitations are now eliminated and should remove barriers to PET payments many providers still encounter. While PET coverage overall has improved, ASNC said some insurance prior authorization policies require previous equivocal SPECT exams, or patients to have a BMI over 40.
An ASNC spokesman told Cardiovascular Business that insurers look to clinical consensus guidelines when constructing their coverage policies. This statement clarifies the consensus of the cardiovascular community.
“In the past, insurers’ policies have too often denied cardiac PET testing unless patients met certain restrictive clinical characteristics,” ASNC President Jamieson M. Bourque, MD, said in a in a news post to ASNC members. “That ends now. This statement confirms that all patients undergoing perfusion imaging are best served by cardiac PET with myocardial blood flow, if available. This is an important step toward ensuring patients have access to the best test.”
Cardiac PET is seeing rapid adoption
Many nuclear cardiology labs have not updated their imaging systems in decades due to slow, minor technology improvements. This was an issue ASNC noted and made a big push following COVID -19 to get centers to upgrade their imaging equipment to take advantage of newer technologies, especially PET. Sales of PET-CT systems have seen a noticeable uptick over the past couple years. Most major imaging system vendors showcased their PET-CT systems at recebt Radiological Society of North America meetings, specifically targeting the growing cardiac PET buyers.
Another big factor driving PET adoption has been the FDA's clearance of the radiotracer flurpiridaz in September 2024. Numerous cardiac imagers predicted flurpiridaz will pave the way for an expansion of PET adoption. The FDA clearance of was considered a paradigm shift for cardiac PET because it can be ordered and delivered in unit doses on demand from regional radiopharmacies. This made PET more attractive economically for imaging centers with low cardiac volumes. Prior to flurpiridaz, rubidium-82 generators were available, but cost approximately $40,000 per month.

Dave Fornell has covered healthcare for more than 17 years, with a focus in cardiology and radiology. Fornell is a 5-time winner of a Jesse H. Neal Award, the most prestigious editorial honors in the field of specialized journalism. The wins included best technical content, best use of social media and best COVID-19 coverage. Fornell was also a three-time Neal finalist for best range of work by a single author. He produces more than 100 editorial videos each year, most of them interviews with key opinion leaders in medicine. He also writes technical articles, covers key trends, conducts video hospital site visits, and is very involved with social media. E-mail: [email protected]